Q and A

| Q and A |
|
|
|
September 2008
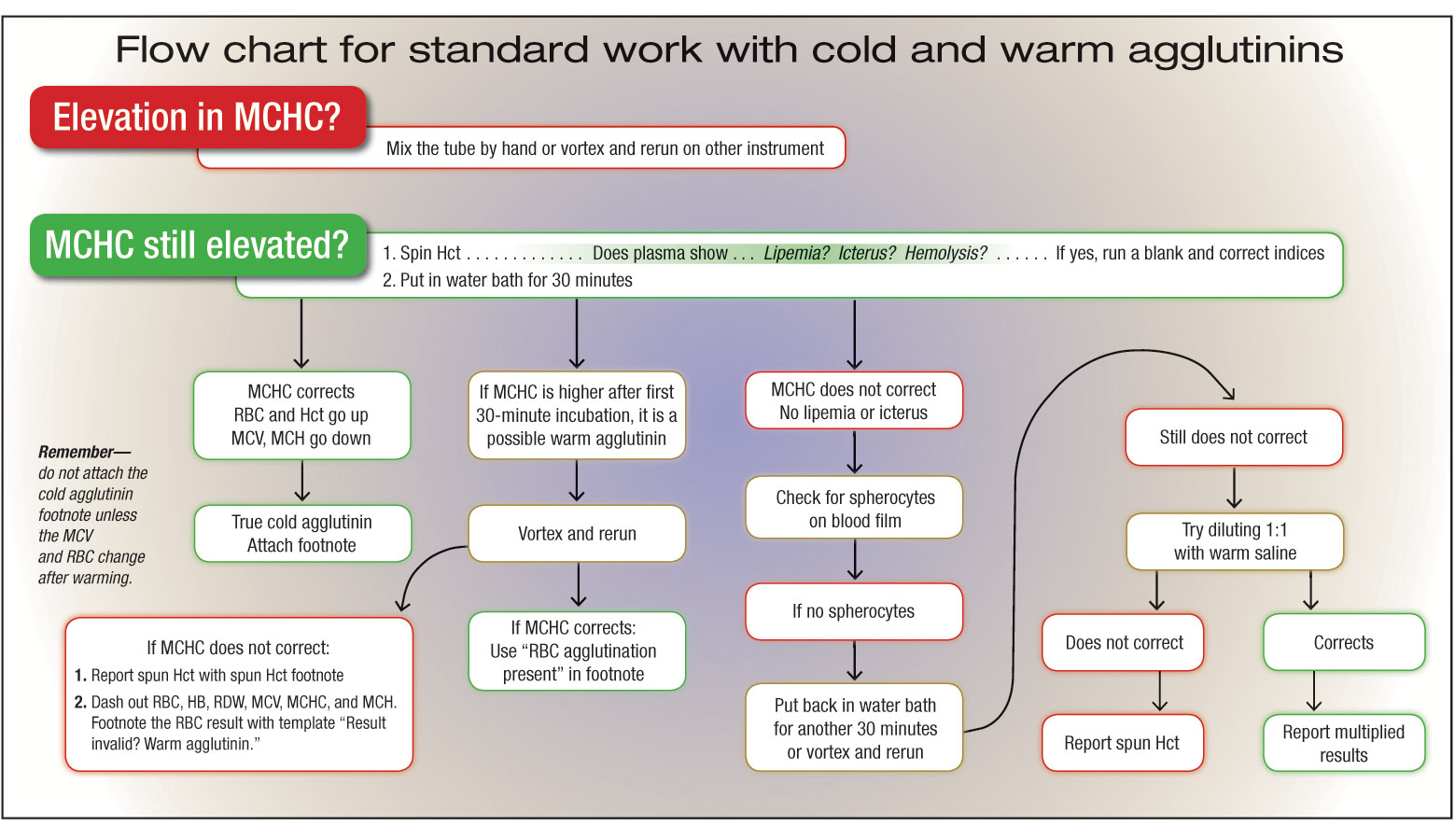
A. Erythrocyte agglutination secondary to a cold agglutinin can interfere with results on automated counters, especially the mean cell hemoglobin concentration, or MCHC (often high).1 The autoantibodies cause micro-aggregates that the instrument may measure as single cells, resulting in low RBC counts and high MCV and MCH results as well.2 Hemoglobin concentrations are still measured reliably. However, because hematocrit is a calculated parameter from the MCV and RBC count on some instruments, it will be unreliable in this setting, as will the MCH (hemoglobin/RBC count) and MCHC (hemoglobin/hematocrit). This effect can be reversed by warming the sample and repeating the test when cold agglutinins are suspected. If the effect is still present, a manual-spun hematocrit will give a more reliable answer and should be reported. Warm autoantibodies can also cause this effect, but in that situation, the abnormalities will not be reversed by warming.3 Here is algorithm that we use in our laboratory when RBC agglutination is suspected References
Katherine A. Galagan, MD
A. {answer} The critical value for the prothrombin time, or PT, can be reported in seconds or the INR, or both. Establishing the level of the critical value is a process that needs to occur at the local level. In this case, it appears that the critical level for the PT in seconds has been set in the laboratory at a level too low, apparently within the therapeutic interval for oral anticoagulant, or OAC, therapy. Setting the level this low may defeat the purpose of the critical value notification, the goal of which is to alert the clinician to a result that is potentially life-threatening, indicating the need for urgent intervention. A PT/INR within the therapeutic interval in a patient taking an OAC is the desired outcome. Calling the critical value too often, and at a level that is desired (therapeutic), will be a bit like crying wolf too frequently and frustrate clinicians. A part of the problem may be the “tradition” from two or more decades ago of setting the critical value for the PT in seconds at a value of 30 seconds. With the insensitive reagents used in the past, 30 seconds was a reasonable value because the upper limit of the therapeutic interval for OAC was com-monly approximately 25 seconds. The International Sensitivity Index, or ISI, of reagents in use in North America at that time was commonly 2.5 or above—very in-sensitive reagents. The -sensitivity of the new reagents now common-ly used is greater (lower ISI). An international recommendation for the sensi-tivity of the thromboplastin is now 0.9 to 1.7, with most laboratories using a reagent with an ISI near 1.0. When using a sensitive reagent like this, a patient with an INR of 3.0 (the upper limit of the OAC therapeutic interval) would have a corresponding PT of 36 seconds, assuming the mean of the reference in-terval is 12 seconds. With a sensitive reagent, a critical threshold of 30 seconds would be too low. Literature documenting the Seventh American College of Chest Physicians Conference on Antithrombotic and Thrombolytic Therapy contains recommendations for therapeutic intervention in OAC patients who have an INR elevated to 5.0 or greater. For this reason, many laboratories have chosen an INR of 5.0 as a critical value for the INR. In 2000, the CAP Coagulation Resource Committee surveyed lab-oratories regarding their coagu-lation practices. One of the committee’s survey questions, to which 604 laboratories responded, addressed the level of the INR used as a critical value. For the responding laboratories, the most frequently chosen INR for the critical value was 5.0 (166 laboratories or 27 percent). The next most common INR critical values chosen were 4.0 (94 laboratories or 16 percent) and 6.0 (74 laboratories or 12 percent). Many other values were chosen, each by a very small number of laboratories. Using the newer reagents with a low ISI, the laboratory may need to adjust substantially the critical value of the PT in seconds. Using the example above of a reagent with an ISI of 1.0 and a mean PT of 12 seconds, the corresponding critical value for the PT in seconds would be 60 seconds, if the value were to be equivalent to the INR value of 5.0. Keeping the values equivalent may be prudent if a critical value for the PT in seconds and for the INR are both being used. References
John D. Olson, MD, PhD |

{kind=link}