Celiac disease testing—sifting through the options

| Celiac disease testing—sifting through the options |
|
|
|
October 2012 Anne Ford Bread. Brownies. Pancake mix. Pasta. Greater public awareness of celiac disease has brought about an impressive number of gluten-free foods on grocery-store shelves and specialty Web sites, giving consumers myriad options. Physicians who want to test patients for celiac disease have numerous possibilities too—so many that the situation might sometimes feel to busy clinicians like too much of a good thing. “You might say, ‘It’s great to have all these options. So why is that so much a problem?’” said Melissa Snyder, PhD. “Basically what happens is that it can or will, depending upon your perspective, lead to over-utilization or inappropriate ordering of the lab tests.” Dr. Snyder, who is director of the Antibody Immunology Laboratory in the Division of Clinical Biochemistry and Immunology at the Mayo Clinic in Rochester, Minn., made those comments during “Testing Algorithms for the Diagnosis of Celiac Disease,” a talk she gave in July at the American Association for Clinical Chemistry meeting. In her remarks, she reviewed the etiology of the disease and the lab testing options, and presented Mayo’s laboratory-driven testing algorithms. Her hope: that her listeners would learn “there are different approaches you can take to dealing with test utilization issues in testing for celiac disease,” she said. “The laboratory can really play an active role in aiding clinicians.” As Dr. Snyder reminded her audience, celiac disease has both genetic and environmental components. In most cases, patients with celiac disease have the HLA-DQ2 allele, the HLA-DQ8 allele, or both. These alleles predispose an individual to developing celiac disease, although just because either of these alleles is present does not mean that person will develop celiac disease during his or her lifetime. However, in some patients with this genetic predisposition, consumption of cereal grain protein, such as that found in wheat, may induce an inflammatory response that damages the small intestinal villi and clinical presentation of celiac disease.
Testing options for celiac disease fall into two categories: serological and genetic. “The serologic tests that we commonly think about for celiac disease are the endomysial antibodies, the tissue transglutaminase antibodies, and the gliadin antibodies,” Dr. Snyder said. Endomysial antibodies (EMA) take their name from the fact that “it was shown on immunofluorescence that if you took patients with celiac disease and exposed their sera to the tissue slices, you would find they had an antibody that stained the connective tissue that surrounds the smooth muscle fibers.... That’s known as the endomysium, so hence the term ‘anti-endomysial antibodies.’ “Immunofluorescence is still used for anti-endomysial antibodies,” she continued. “But anytime you have an immunofluorescence test, really what you want to know is: What is the specific antigen that the antibody is binding to within that tissue structure? And ultimately it was found out that anti-endomysial antibodies are actually binding to the antigen tissue transglutaminase (tTG). So that then led to the development of tTG antibody testing, and this is primarily done using enzyme immunoassay.” In other words, the EMA test and the tTG test use different methods to look for the same antibody. As for the gliadin antibodies, “you can have an unmodified gliadin, which is used as the antigen, or you can have the deamidated gliadin as the antigen,” Dr. Snyder noted. Gliadin is made from taking an ethanol fractionation of gluten, with gliadin being the ethanol-soluble fraction of gluten. “You just take the gliadin that you extract from that ethanol fraction, and you then use that as the antigen for the enzyme immunoassay. So that’s what we would call unmodified gliadin. Then you have the deamidated gliadin antibodies, which are antibodies to gliadin peptides that have been deamidated.... And they’re using that as the capture antigen in the enzyme immunoassay.” As useful as serology testing for celiac disease can be, it comes with a number of caveats, Dr. Snyder warned. The first: the issue of selective IgA deficiency. “Many people go through life having a selective IgA deficiency, and they never realize it,” she said. “The problem is, if you’re evaluating someone with celiac disease, you need to be aware of a selective IgA deficiency.” First, because it’s more common in people with celiac disease than in the general population, for reasons that are unclear. And second, because when using the EMA or the tTG test, “you can look for either the IgA or the IgG antibody. Those are the clinically relevant isotypes for the autoantibodies. So if you have a patient with a selective IgA deficiency, obviously testing them for IgA antibodies is not going to be very useful.” Then, too, physicians should be aware that many patients who suspect they have celiac disease put themselves on a gluten-free diet before they even walk into a doctor’s office, in which case their autoantibody production may be suppressed. “So you may have a situation where a patient is on a gluten-free diet, they come in for serology testing, and it’s negative. And you don’t know if that’s the effect of their gluten-free diet, or if they just didn’t have celiac disease.”
Turning her attention to the genetic side, Dr. Snyder reminded her listeners that HLA-DQ2 and HLA-DQ8 are MHC class II molecules, and that “you have to have both an alpha and a beta chain to have a functional class II molecule.” Thus, when testing for DQ2 and DQ8, a laboratory must look at both the alpha and beta chains. To be considered truly at risk for celiac disease, a patient must be heterozygous for HLA-DQA1*05 and DQB1*0201, homozygous for DQA1*0201 and DQB1*0202, or heterozygous for DQA1*03 and DQB1*0302. (Whereas if a patient is heterozygous for DQA1*0201 and DQB1*0202, “there’s conflicting reports in the literature whether it’s associated with celiac disease or not.”) If a patient is negative for DQ2 and DQ8, celiac disease can more or less be ruled out. And if the patient is positive? Then that’s “consistent with a possible diagnosis, so the patient has the genetic predisposition for the disease,” she said. “However, given that about 30 percent of most populations are DQ2 or DQ8 positive . . . you’re going to have a lot of patients who are DQ2 or DQ8 positive, yet do not have active celiac disease at that given point in time.” So which test or combination of tests is most effective in diagnosing celiac disease? After all, Dr. Snyder pointed out, you want to make sure that a patient who is unlikely to have celiac disease is not subjected to a confirmatory biopsy of the small intestine. To determine the best testing option, she turned to a study co-authored by Mayo gastroenterologist Joseph A. Murray, MD, pathologist Henry A. Homburger, MD, and colleagues (Rashtak S, et al. Comparative usefulness of deamidated gliadin antibody measurements in the diagnosis of celiac disease. Clin Gastroenterol Hepatol. 2008;6:426–432).
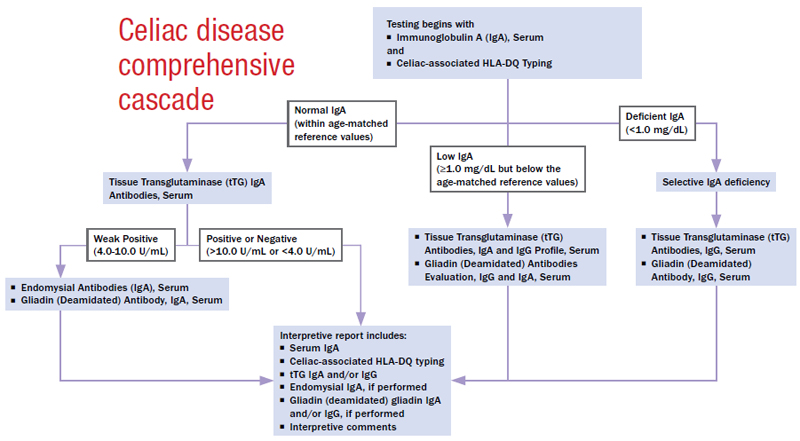
The study determined that EMA-IgA had 99 to 100 percent specificity when using umbilical cord and monkey esophagus tissue substrate. Sensitivity was 86 to 93 percent when using umbilical cord and 96 to 99 percent with monkey esophagus. Meanwhile, anti-tTG-IgA had 93 to 97 percent specificity when using purified guinea pig tTG and 96 to 99 percent specificity with recombinant htTG; sensitivity was 81 to 90 percent with purified guinea pig tTG and 90 to 100 percent with recombinant htTG. Finally, anti-tTG-IgG had 94 to 100 percent specificity when using purified guinea pig tTG but was only 36 to 54 percent sensitive. “That’s why the IgA isotype is generally considered to be the better test to use for screening, although you do have to again be aware of that total IgA deficiency issue,” Dr. Snyder said. To examine the performance of gliadin, she turned to a different study (Rostom A, et al. The diagnostic accuracy of serologic tests for celiac disease: a systematic review. Gastroenterology. 2005;128:S38–46), which found that deamidated gliadin IgA had 95 percent specificity and 74 percent sensitivity, while deamidated gliadin IgG had 98 percent specificity and 65 percent sensitivity. In comparison, unmodified gliadin IgA was only 90 percent specific and 63 percent sensitive, with unmodified gliadin IgG being 90 percent specific and 42 percent sensitive. To summarize: “tTG-IgA and deamidated gliadin-IgA probably have the best combination of sensitivity and specificity for diagnosis,” Dr. Snyder said. “EMA-IgA has excellent specificity, although it might have a slightly lower sensitivity. tTG-IgG and deamidated gliadin-IgG have poorer overall sensitivity; however, they can be useful in the context of patients who have that selective IgA deficiency. And then you have the unmodified gliadin-IgA and IgG, which, in comparison to all the other tests that are available, have poorer sensitivity and specificity. And then, if you look at the genetic test, the genetic test is useful for ruling out celiac disease, but not necessarily for establishing a diagnosis.” “There’s a lot to take in here as far as comparing the different antibodies, the different isotopes, and really what’s most appropriate,” she concluded. “And it can be a lot for clinicians to keep straight.” Pathologists can help clinicians wade through their testing options for celiac disease in several ways, for example, by having tTG come up as the first option when a clinician performs a search for celiac disease in an electronic ordering system, providing direct feedback to physicians who consistently order redundant tests, or by simply discontinuing tests that don’t perform well or have low clinical value. At Mayo Clinic, the laboratory decided to do two things: first, discontinue unmodified gliadin testing for both IgA and IgG (once deamidated gliadin became available, she said, “we felt there was no reason to keep gliadin as an orderable test”); and second, implement testing algorithms for celiac disease. “We decided we wanted to try to take the bull by the horns,” Dr. Snyder said. The Mayo team came up with an algorithm it calls the “comprehensive cascade.” It works like this: The laboratory needs two samples from the patient: serum for serology testing and a whole blood sample for HLA typing. When the laboratory receives those two samples, the HLA typing is performed up front, and then the total IgA is performed. “The total IgA is done because of that issue with selective IgA deficiencies. So if the patient has normal IgA based on the reference ranges we had established within the laboratory, then we reflex to performing a tissue transglutaminase IgA-only antibody test,” she said.
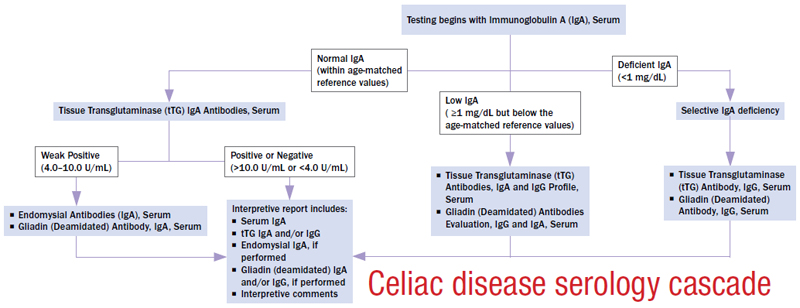
If that test result is positive and the permissive HLA alleles are present, the patient may have celiac disease, and a biopsy may be indicated. If the result is negative, the high sensitivity of tTG IgA is likely sufficient to rule out celiac disease as a diagnosis for most patients. “So [for] most patients, when this test is ordered, only those three tests [HLA typing, total IgA, and tTG IgA] are performed,” she said. However, if the patient result falls into the range established as equivocal by the tTG test manufacturer, two additional tests are added: EMA-IgA and anti-deamidated gliadin IgA (assuming the patient is IgA-sufficient). “We use these two tests in combination with the HLA typing to try to sort out what is the meaning of this equivocal total anti-tTG-IgA antibody,” Dr. Snyder said. “It allows us to provide a little bit more of an interpretation regarding the test results.” What if the patient has a selective IgA deficiency? Then the laboratory reflexes to performing tTG-IgG and deamidated gliadin-IgG. “We use both of those antibodies as opposed to just one, because they both have somewhat lower sensitivity,” Dr. Snyder noted. As for the patients who have some detectable total IgA yet fall below the reference range for their particular age group, “the IgA testing may be useful, but it still might not be sensitive enough,” she said. For those patients, the laboratory performs four tests: TTG-IgA and IgG as well as deamidated gliadin IgA and IgG. “We could just do the IgG, but we thought because they have somewhat lower sensitivity, and because these patients do have some IgA, the IgA antibodies might have some diagnostic utility.” After creating the comprehensive cascade, Dr. Snyder and her team realized they might encounter patients who had had HLA typing done and already knew they were DQ2- or DQ8-positive—“in which case, we certainly wouldn’t want them to have to be retested, because they’re not going to change in their HLA type,” she said. “So we basically took that first algorithm that we had and just left out the HLA typing. . . . So in this case, you would just have what we call the serology cascade. The active reflexing that occurs in this cascade is identical to the comprehensive cascade.” The third and final cascade the Mayo team created is for patients on a gluten-free diet. “In this case, we do one test up front, and that is the HLA-DQ typing,” Dr. Snyder said. If the patient is negative, no further testing is needed. If the patient is positive for DQ2, DQ8, or both, then the serology testing is performed, specifically a total IgA along with tTG-IgA and IgG, as well as deamidated gliadin-IgA and IgG. Why? Because “the sensitivity of each of those individual tests is going to be lower in these patients because of that gluten-free diet,” Dr. Snyder pointed out. “Therefore, in order to maximize the sensitivity of this part of the reflex cascade, we ended up adding on the testing for all four of the specific autoantibodies … to not miss any patients who we know are DQ2-positive but yet are following that gluten-free diet. If any of those results are positive, then we would say it is consistent with celiac disease and certainly could be confirmed by biopsy, if that’s desired by the clinician. If all the results here are negative, it’s still possible that the patient has celiac disease because we know they are DQ2- or DQ8-positive, but because of the gluten-free diet, perhaps their serology is negative.” At that point, the clinician would decide whether to have the patient undergo a gluten challenge. In response to an audience member’s question, Dr. Snyder noted that at Mayo, each test within the various algorithms is available to order individually. That’s because clinicians monitor the immunologic response of patients with celiac disease “by looking for the tTG antibodies or whatever the patient happened to be positive for,” she said. “The patient comes in. They say they’re feeling better. But they’re still going to get the antibody test ordered.” Anne Ford is a writer in Evanston, Ill. |