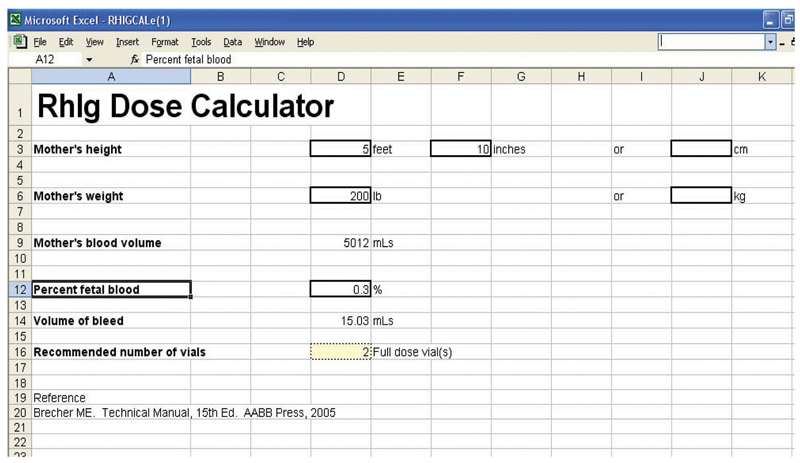
Bringing new rigor to RhIG calculations

| Bringing new rigor to RhIG calculations |
|
|
|
May 2008 Anne Paxton Start with a medical event that has only a three-in-1,000 chance of occurring. Throw in a 50-year-old laboratory test with less than perfect accuracy, an intervention that is not able to be calculated precisely, and adverse outcomes that may not come to light for months or years, and you are likely to get confusion. And that’s exactly what many laboratories are experiencing when they test Rh(D)-negative mothers for fetomaternal hemorrhage (FMH) to determine the proper dose of Rh immune globulin (RhIG) after birth of an Rh(D)-positive child. In two recent proficiency testing surveys, when the CAP asked laboratories how many vials of RhIG they would recommend giving based on the tests, “We were amazed at the broad diversity of answers we saw,” says James AuBuchon, MD, chair of pathology at Dartmouth-Hitchcock Medical Center, Lebanon, NH. “We recognized there was clearly a lack of uniformity and lack of optimum practice in the field.” To address this variability, the CAP’s Transfusion Medicine Resource Committee, to which Dr. AuBuchon is an advisor, has developed a special RhIG dose calculator. The committee hopes physicians can use it to avoid a miscalculation that, within the universe of rare events, could be fairly common.
In fact, obstetrical delivery services administer RhIG routinely to hundreds of thousands of mothers in the United States. Some 16 percent of mothers are Rh-negative, and 60 percent of their babies will be Rh-positive, explains Mark E. Brecher, MD, vice chair of the Department of Pathology and Laboratory Medicine at the University of North Carolina and a member of the CAP committee. So more than half of all Rh-negative mothers will need at least one dose of RhIG to provide prophylaxis against alloimmunization to the D blood group antigen. For most mothers, one vial (300 µg) of RhIG is sufficient to cover that pregnancy. “Basically one dose will cover 15 mL of red cells or roughly 30 mL of whole blood spilled by the baby,” Dr. Brecher says. The problem arises when there is significant fetomaternal hemorrhage, which can be caused by abdominal trauma, vaginal bleeding, ectopic pregnancy, fetal death, or invasive obstetrical procedures, though many episodes of FMH are not associated with a clinical risk event. “In the small percentage of cases where there is an FMH, about 0.3 percent, you’ll need more than one dose, and that’s where the calculation is most important,” Dr. Brecher says. “You do a screen on maternal blood after delivery, most commonly using the fetal rosette screening test, which checks to see if any Rh-positive fetal blood cells are circulating in maternal blood. If that’s positive, you go on to a quantitative test of the bleed.” Based on the quantitative results, laboratories can follow the recommendations RhIG manufacturers provide in package inserts as well as those in the literature provided by experts in the field. “But no one knows which is the best algorithm,” he notes. “Each algorithm is generally designed to supply a surplus of RhIG to make sure you don’t underdose.” “I don’t think anyone would say one method is clearly superior to another, but most people use the method outlined in the AABB Technical Manual,” says Dr. Brecher, who is editor of the current edition of the manual. The CAP conducts a twice-yearly proficiency testing program surveying laboratory performance of fetal red blood cell detection. Participants can screen specimens and determine the percent of fetal RBCs in the maternal blood sample using a staining method or flow cytometry. Then they report the number of doses of RhIG they would recommend based on the quantitation. Because of an apparent lack of consistency, supplementary questions were added in 2006 and 2007 about the laboratory’s test method and RhIG dose calculation method. “We would normally ask how many vials of RhIG the laboratory would give for the examples in the proficiency testing exercises, and we would get some responses that said no vials would be necessary, even though we were setting up questions such that, with an Rh-positive baby, the mother should have gotten at least one vial,” says former transfusion committee member Glenn Ramsey, MD, professor of pathology, Northwestern University Feinberg School of Medicine, Chicago. “We didn’t know quite what to make of it. Yes, it is a little tricky in terms of putting the numbers into a formula, but it’s not that complicated,” Dr. Ramsey says. “And we decided to do these extra questions to explore the accuracy of the dosage recommendations that hospitals and transfusion services would suggest.” In the first investigation, nearly 1,600 laboratories were surveyed on their accuracy, and to the surprise of the Transfusion Medicine Resource Committee members, 9.2 percent of the 783 that used the AABB Technical Manual calculation method recommended too low a dose of RhIG. Sixty-six recommendations were one dose too low, two were two doses too low, and four were three or more doses too low. In the second survey, the committee provided four calculation exercises and found that in three of them, 21 percent to 30 percent of laboratories underestimated the necessary dose of RhIG, usually by one dose. “First we thought we hadn’t explained it carefully enough,” Dr. AuBuchon says. The standard formulas, he notes, usually do not take into account the size of the patient; most of them assume an arbitrary patient size. “If the mother is at the upper end of the scale in terms of size, the volume of fetal blood might be substantially underestimated.” “So we kept going at this stepwise, thinking if we just make one more piece of information clearer, then the labs will get it right. We said, ‘Let’s say how large the mother’s blood volume is,’ but there was still a huge diversity of responses, even when we specified use of the AABB Technical Manual method. When we literally gave a formula and all the numbers to plug in, they still didn’t come up with the same number. “So that drove us to say, ‘Let’s provide them with a foolproof method,’” Dr. AuBuchon says. Dr. Ramsey led the write-up of results, which have been submitted for publication in the Archives of Pathology & Laboratory Medicine, but the committee felt it was important for more general audiences to know about the findings as well. In reviewing the literature, he says, “We couldn’t find any other study elsewhere regarding laboratory dosage calculations. Others have seen problems in the logistics of giving the dose, or the dose not ordered or tests not being sent to the lab, but I couldn’t find any other information about laboratory accuracy on these recommendations.” The responsibility for determining RhIG dose is often shared. In some hospitals, obstetricians are involved directly in RhIG calculations, but the pathologist is the key player equally often. “Ultimately this is something given to a patient, so there has to be a physician order somewhere in the process, but how much involvement the obstetrician has is variable,” Dr. AuBuchon says. At Dartmouth-Hitchcock Medical Center, there is a standing order for the mother to receive the appropriate dose of RhIG as determined by the laboratory. “We send up the dose and the nursing staff administers it, and the obstetrician is probably not directly aware of the calculation because we’ve done it for them,” he says. “In some institutions, the lab just generates the proportion of fetal cells in maternal circulation and the obstetrician decides how much RhIG to give, but I think that’s unusual.” In practice, says S. Gerald Sandler, MD, director of transfusion medicine at Georgetown University Hospital, Washington, DC, neither pathologists nor obstetricians have a high volume of experience with this calculation. “This calculation is subject to human error because it is performed infrequently,” he says. Less than 50 years ago, the discovery of the cause of Rh hemolytic disease of the newborn was followed quickly by the development of an effective treatment (exchange transfusion) and prevention (Rh immune globulin), Dr. Sandler notes. Medical science has not uncovered how the phenomenon of passive immunization works. “It’s really a paradox—we prevent a woman from forming potentially harmful anti-D by giving her an injection of anti-D (RhIG) from another person,” he says. But as early as 1943, Philip Levine observed that if a first Rh-positive newborn had red cells compatible with the mother, there was Rh alloimmunization at a much higher rate than if the ABO(H) antigens were incompatible with the mother, Dr. Sandler, a member of the transfusion committee, says. “Traditionally, physicians believed that fetal red blood cells didn’t circulate in the mother’s blood—unless there was some disruption and particularly at delivery if there was a fetomaternal hemorrhage, which is the major cause of alloimmunization to the D-antigen. But we now know that at 28 weeks and afterward there may be sensitization, so the current practice is at 28 weeks an Rh-negative mother is given an injection of RhIG to protect her for the rest of her pregnancy.” The consequences of a mistake in dosing can be serious. Once the mother has become alloimmunized, Dr. Sandler says, “nothing can undo it.” As with any severe medical problem, the outcomes for the mother’s future fetuses will vary. “Prior to the preventive strategy, there was a certain number of Rh-positive children—not the first ones because they were the ones who stimulated the mother—but starting with the second and subsequent children. They were stillborn, or they had heart failure due to anemia and died, or they had high concentrations of bilirubin that couldn’t be metabolized and led to a wide range of damage to the nervous system.” In 1946, Harry Wallerstein performed the first successful exchange transfusion to treat Rh hemolytic disease of the newborn, and it has remained the standard therapy since, Dr. Sandler says. “But hemolytic disease is largely history in the U.S. We’ve gone from approximately 13 percent to 0.1 percent. So now, only one in a thousand newborns who are Rh-positive born to an Rh-negative mother will have this problem.” Alloimmunization does not guarantee a bad outcome for the mother’s next pregnancy, and there are mechanisms by which obstetricians can intervene as appropriate to make sure the pregnancy has a successful outcome, Dr. AuBuchon says. “But it will at least cost more to take care of the woman in the next pregnancy, and could even potentially change someone’s decision about becoming pregnant again, if they recognized they had become alloimmunized and were with the same partner.” For most Rh-negative women by far, the qualitative screen is negative, and one vial of RhIG will be more than adequate to cover the normal 30 mL of fetal blood in maternal circulation. The RhIG dose calculator comes in when the screening result is positive and a quantitative test has to be done, most typically the Kleihauer-Betke assay. Developed in 1957, it is one of the oldest laboratory tests still used. “It’s tedious, prone to error, and quite inaccurate,” Dr. Sandler notes. “In fact, it’s so inaccurate that under the current recommendations—and this is built into the calculator—when you have calculated the number of vials to give the mother, you add another vial for a margin of safety because we all question whether the method is accurate enough to rely on.” However, most hospitals, because they don’t have flow cytometry readily available, continue to use the Kleihauer-Betke method. “The current recommendation is to give the injection of RhIG within a 72-hour period following delivery,” Dr. Sandler says. “If you send the sample out to a reference laboratory and the result doesn’t come back before the mother is discharged, there’s a risk of overlooking the injection, whereas if you take the sample to the hospital’s laboratory and say, ‘What’s the result?’ you can go back upstairs and the nurse will get the injection done.” In Dr. Sandler’s opinion, many hospitals continue using the Kleihauer-Betke test because of this time-related chain-of-responsibility issue. Adding another layer of imprecision to the alloimmunization prevention strategy is the source of the 72-hour rule: a 1960s experiment that could not ethically be repeated in the 21st century, Dr. Brecher says. “When they were doing the first studies on RhIG preparation, they used ‘volunteers’ from Sing Sing prison. They transfused various amounts of Rh-positive red cells and, in the following days, gave them various doses of RhIG to see what stopped them from forming immune responses.” But since researchers were allowed into Sing Sing only from Monday to Friday, there was a subgroup that got an injection of red cells on Friday but only received RhIG on Monday. “And it’s from that subset that we came up with the 72-hour rule,” Dr. Brecher says. It is accepted in the literature that there is a certain proportion of RhIG failures, in which an Rh-negative mother with an Rh-positive fetus receives RhIG that fails to prevent alloimmunization. But to Dr. AuBuchon’s knowledge, a retrospective study, examining the patient charts of 100 women in the failure category and recalculating how much immune globulin they should have been given to see whether that was the problem, has never been done. “That would be scientifically very interesting,” he says. At a cost of about $90 a vial, RhIG is not exceedingly expensive, and overdose is not considered a major risk, he points out. But essentially RhIG has been produced from the plasma of individuals found to have anti-D, and the supply is limited. “Those may be women, but most of the donors are men who are actually immunized with Rh-positive blood cells. So there are not a lot of these people,” Dr. AuBuchon says. “And there are some risks of potential alloimmunization because of being exposed to other people’s red cells. No one would want to propose using it in situations where it’s not medically appropriate.” Dr. Sandler, who took responsibility for the CAP fetal RBC proficiency test survey this year, says the CAP has no recommendation on whether to use flow cytometry in place of the Kleihauer-Betke test. “We will continue to encourage laboratories to transition from the older method because flow cytometry is more accurate and it is the test of the future. However, not all hospitals have the technical skills or equipment for flow cytometry, and it is not fiscally justifiable to introduce that technology solely for this infrequently required test.” With flow cytometry’s greater accuracy, Dr. AuBuchon says, “you could get away with not having to put a fudge factor or a cushion into the equation.” Conveniently, his own hospital has a flow cytometry laboratory down the hall from the transfusion service. But logistically it would be difficult for many hospitals to add flow cytometry in-house, and if it is in-house, the instrumentation is likely to be in hematology rather than in the transfusion service. Members of the Transfusion Medicine Resource Committee say the CAP is providing the RhIG dose calculator as a service to members, to minimize errors that might occur because of miscalculations. Dr. Sandler suggests that laboratories put an RhIG calculator “widget” icon on their computer screens. “Pathologists should use it whenever it’s their responsibility to calculate the correct dose of RhIG, to ensure that this uncommon but very important calculation is performed accurately.” In a disclaimer that the committee has issued for the RhIG dose calculator, it cautions that the calculator is only one resource, use by pathologists is voluntary, and it does not necessarily ensure a successful medical outcome. Pathologists “should apply professional judgment to the specific clinical circumstances presented by the individual patient or specimen,” the committee says in the disclaimer. It also encourages pathologists to document the reasons for use of a particular algorithm, procedure, or test—whether or not it is in conformance with the calculator—and to consider other relevant medical and scientific information that becomes available after the calculator’s publication date. Nevertheless, laboratories should make sure the calculation is standard operating procedure and that it’s done correctly, Dr. AuBuchon believes. “Even if they don’t use it every time, at least if they do their calculations for the next 10 samples they get the usual way, then check them against the College’s calculator to see if they are coming up with the same number, they can validate their method.” Says Dr. Ramsey: “It’s just too important a calculation to get it wrong.” Anne Paxton is a writer in Seattle. The dose calculator can be found at www.cap.org, under Committees and Leadership, Transfusion Medicine Resource Committee, Transfusion Medicine Topic Center. |
|
||||