 CAP TODAY Pathology/Laboratory Medicine/Laboratory Management
CAP TODAY Pathology/Laboratory Medicine/Laboratory Management

Karen Titus
July 2016—Time was running out for Yuri Nikiforov, MD, PhD, vice chair for molecular pathology and division director of molecular and genomic pathology, University of Pittsburgh Medical Center.
For nearly a year he had been working to assemble an international group of experts—pathologists, endocrinologists, a surgeon, and, unusually, a psychiatrist and a patient advocate—to discuss that most vexing of thyroid tumors, encapsulated follicular variant of papillary thyroid carcinoma, or EFVPTC.
“Way overdue” is how many see the nomenclature revision for noninvasive encapsulated follicular variant of papillary thyroid carcinoma, says Dr. Yuri Nikiforov (right), with Dr. Sally Carty and Dr. Raja Seethala at UPMC.
Their goals were less ambiguous than the tumor: to evaluate clinical outcomes, refine diagnostic criteria, and develop a new nomenclature. No detail was too small, and nothing was left to chance. Prior to the meeting, “We had collected a large number of EFVPTC pathological samples”—265 patients with noninvasive or invasive tumors—“and the cases were distributed and reviewed by 24 pathologists,” Dr. Nikiforov says. This was followed by eight weekly, one-hour teleconferences to review the difficult cases and discuss opinions and consensus criteria, all prior to the day-and-a-half, face-to-face meeting in Boston in March 2015.
At the conference, participants learned the blinded results of the follow-up. All 109 cases that were called noninvasive were highly indolent. The invasive EFVPTCs, on the other hand, were quite aggressive. That review took most of the day. “And at the end of the day, we started to discuss a new name for the tumor,” Dr. Nikiforov says. Carcinoma in situ? Follicular adenoma? Noninvasive follicular thyroid neoplasm?
Round after round went the discussion and voting, like an Iowa caucus, into the evening. “We could not decide,” says Dr. Nikiforov.
Work resumed the next day. The clock was ticking. “We had to end the conference at noon,” he remembers. Finally, “At 11:30, we reached a consensus.”
Behold noninvasive follicular thyroid neoplasm with papillary-like nuclear features, or NIFTP (Nikiforov YE, et al. JAMA Oncol. Published online April 14, 2016). Though it’s not part of any official guideline, it’s likely here to stay, for better (say many), possibly for worse (fret a few detractors), or to little effect at all (shrug some).
The name is notable for what it lacks: the words “carcinoma” and “cancer.” The presentation by Guy Maytal, MD, medical director, ambulatory psychiatry, Massachusetts General Hospital, and assistant professor, psychiatry, Harvard Medical School, influenced many to steer clear of these words, given their impact on, among other things, patients’ psyches. As a medical-geometry truism, in patients’ minds the shortest distance between diagnosis and death is “cancer.”
But the change began several years before the Boston meeting, as a notion, a whisper of sorts, at the end of a prior research effort. The Cancer Genome Atlas project mapped the somatic mutational landscape of the most common types of papillary thyroid carcinomas and showed that PTC fundamentally consists of two types of tumors, those that are driven by RAS and those driven by BRAF. (See “Thyroid cancer: In a flourish of subtypes, genes, and drivers,” CAP TODAY, January 2015.) “That laid the foundation for us thinking about these follicular tumors,” says TCGA project co-chair Thomas Giordano, MD, PhD, who was also part of the most recent effort. Some pathologists even suggested the encapsulated type might be given a new name, and noted that FCIS was already being used by some.
Dr. Nikiforov predicted at the time that a name change could indeed happen—but only after much time and wrangling. Thus he’s pleased the wait turned out to be relatively short, at least in medical years. Looking at this most recent conference and paper, he says, “It’s remarkable. I can tell you honestly, the task was humongous.”
Adds Virginia LiVolsi, MD, who participated in both studies: “‘Quick’ can be defined in various ways. In medicine, two years is not that bad.” Dr. LiVolsi is a professor of pathology and laboratory medicine, University of Pennsylvania Perelman School of Medicine.
Their work has drawn praise from nonparticipants as well. Sally Carty, MD, says she was impressed the task was accomplished “so rapidly and so elegantly. It’s a brilliant idea,” says Dr. Carty, a professor of surgery and chief, Division of Endocrine Surgery, University of Pittsburgh, and past president, American Association of Endocrine Surgeons.
The study even caught the attention of The New York Times, whose April 15 article stirred interest among patients and physicians in revisiting EFVPTC diagnoses.
The group’s accomplishment was not completely unexpected. Interest in these tumors is considerable, as evidenced by the response to the paper. Dr. Nikiforov reports that in the first three weeks after the study’s publication, 67,000 people looked at the article online. By way of comparison, he says, other, similarly consequential studies might draw 5,000 hits. “The number of emails, questions, and comments I get every day is enormous,” he says. “I’ve received hundreds of emails since the paper came out. Many people say, ‘This is way overdue.’”
Pathologists who see these lesions routinely are all too familiar with the dilemma they pose. Though there is no invasion, they have the nuclear features of papillary carcinoma. So is it benign or malignant?
Not all tumor types pose similar dilemmas. In colorectal cancer, for instance, the spectrum has been well delineated: polyp, dysplasia low-grade, dysplasia high-grade, carcinoma in situ, invasive carcinoma. “In thyroid, we ignored this for many years,” Dr. Nikiforov says. (He could be speaking about Illinois’ state budget.) Though several previous studies had shown prognosis was excellent if these lesions were noninvasive, they were based on smaller series of cases. Consensus diagnostic criteria were lacking, as was methodical, lengthy follow-up. And so it went, “for many years, without resolution,” Dr. Nikiforov says.
It was time for a solid study.
An important part of the study design, he says, is that “we didn’t simply have 24 pathology experts meet and say, ‘In our expert opinion, this should now be benign.’” In the era of evidence-driven medicine, “You cannot do this.”
Among the patients with noninvasive disease, who were followed for 10 to 26 years (median, 13 years), all were alive and had no recurrences or other signs of disease at final follow-up. “None of these tumors was ever heard from again,” as Dr. LiVolsi puts it. In this group, 67 received lobectomy alone, and none received radioactive iodine ablation. The findings correspond with previous studies of noninvasive EFVPTCs. Among 352 such tumors, the authors note, only two recurred. In one case, the tumor had been incompletely excised; in the other, the noninvasive status was questionable.
In the second group, 85 of the 101 patients with invasive disease were treated with radioactive iodine ablation. In one- to 18-year follow-up, 12 had an adverse event, including distant metastases (two of these five patients died of their disease), lymph node recurrence, persistent disease, and detectable serum thyroglobulin, indicating either indeterminate or incomplete response to therapy.
The upshot, the authors say, is that an absence of invasion entails a very low risk and should not be termed “cancer.” Pathologists are no longer forced to decide between malignant and benign—it can be a borderline, pre-cancer lesion, says Dr. Nikiforov. “If the tumor is removed, progression is stopped.” These patients don’t need to be labeled with cancer, and they can avoid completion of thyroidectomy, radioactive iodine therapy, and the cycle of six- or 12-month follow-ups.
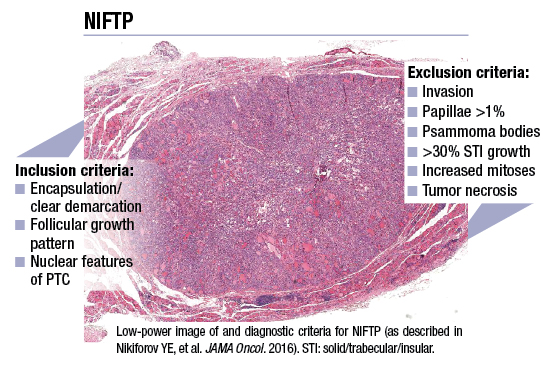
The study offered a set of diagnostic criteria for identifying NIFTP, including lack of invasion, follicular growth pattern, and PTC nuclear features. Since the JAMA Oncology article targets a more general audience—the better to reach clinicians, says Dr. Nikiforov—the authors had limited space to describe pathology-related details in depth. A subsequent article, containing a detailed review of morphology features, is nearly complete. Dr. Nikiforov calls it “a step-by-step guide to making this diagnosis.”
Identifying NIFTP demands scrutiny of the lesion to look for invasion, says Dr. LiVolsi. “The definition of the lesion has to really be perfect for the pathologist to apply this terminology.”
Pathologists need to examine the entire lesion. “I think expert pathologists have been examining the entire capsule for some time. That’s not to say it’s been universally done,” says Gerard Doherty, MD, the Utley professor and chair of surgery, Boston University, and surgeon-in-chief, Boston Medical Center.
If pathologists have not been submitting the entire lesional capsule for histologic interpretation, they need to do so, says Raja R. Seethala, MD, pathologist and director, Head and Neck/Endocrine Pathology Center of Excellence, UPMC. Dr. Seethala says this has been a matter of debate in the past, with practice patterns differing along academic/community lines. “It’s no longer optional to submit the entire capsule,” he says.
For pathologists, “If the lesion is 1.5 cm, that’s not so bad. If the lesion is 4.5 cm, that’s a lot more work,” Dr. LiVolsi acknowledges. Moreover, she adds, some of these lesions might have only one lone focus of invasion. The risk associated with such lesions is still low—but not as low as the risks of lesions now known as NIFTPs, which have no invasion and thus better clinical implications. “So if you do not train pathologists in the importance of examining the entire capsule of the lesion—and if there’s no capsule, the entire perimeter—then we’ve failed,” Dr. LiVolsi says.
Though this is one paper, already it’s making waves. The WHO has accepted the new entity and included it in its new classification of tumors of endocrine organs that will appear in print next spring. “This is a big step,” Dr. Nikiforov says. “It ensures the acceptance of this terminology around the world.”
 Closer to home, individual pathologists are feeling reverberations as well.
Closer to home, individual pathologists are feeling reverberations as well.
Dr. Giordano, the Henry Clay Bryant professor of pathology, University of Michigan, says he was recently asked to re-review a case of a thyroid nodule that was called PTC. “The surgeon was looking for any reason not to be all that aggressive with the patient.” Dr. Giordano sent the paper, in prepublication form, to U-M’s head endocrine surgeon, who “read it, liked it, and discussed it with the patient, then wrote back and said the patient was thrilled to have a justifiable reason not to have a total thyroidectomy and undergo radioactive iodine treatment,” says Dr. Giordano, who is also director of both the Division of Molecular and Genomic Pathology and the UMCCC Tissue and Molecular Pathology Core, Department of Pathology.
In another recent case, the head thyroid endocrinologist at Michigan asked for review of a case involving a patient who’d already undergone a total thyroidectomy, based on a diagnosis of papillary carcinoma and the presence of bilateral nodules. No invasion was noted. The case will be revised to NIFTP, Dr. Giordano says. “That will be a clear signal not to give the patient radioactive iodine” and to regularly check the patient’s thyroglobulin levels.

Dr.Giordano
Revisiting cases presents technical challenges, Dr. Giordano concedes. “If you can’t be confident there isn’t invasion, based on a thorough examination of the entire tumor capsule, you’ll still have to use the old nomenclature.” Not every case can be reviewed, but moving forward, he says, he hopes this will mandate that pathologists sample these nodules more thoroughly.
Using the NIFTP nomenclature could eventually have wide clinical impact, Dr. Giordano predicts, though “It all depends on the clinical group.” While Michigan seems poised to adopt it, “I can imagine other places where people are more comfortable with the more aggressive treatment.” Just as there is interobserver variability among pathologists, so, too, is there variability in surgeons’ practices. “Some like to do total thyroidectomies more than others, even for a traditional papillary carcinoma. There’s a lot of regional variation,” Dr. Giordano says.
Regardless, he’s joined the chorus of physicians who call the move “long overdue.” Over the years, he says, “Pathologists have gotten a little too aggressive with these tumors. We focused more on the nuclear features, and less on whether the tumor was invasive. And I think the true malignant potential resides in whether the tumor’s invasive.”
In the first case he mentioned, Dr. Giordano notes, the likelihood of the patient’s tumor becoming a metastatic cancer “is not zero, but it is really close to zero. So what we’re trying to do is balance all that extra surgery, all that radioactive iodine, for tens of thousands of patients—maybe more, globally—versus the rare patient who may still develop a clinically significant cancer.” It can be a tough decision, he concedes. “Because people want to be absolutely certain.” While noninvasive tumors only rarely behave like cancers, he says, there are examples of follicular adenomas that metastasize.
When this occurs, it’s not unusual for these to be considered a mistake on the part of the pathologist. The fact is, “There is always some built-in sampling error.” As a result, “Every endocrinologist will tell you about their one or two patients” who had what turned out to be follicular carcinoma, rather than, as thought, a follicular adenoma.
“Is that going to happen with NIFTP? Probably,” says Dr. Giordano, launching into a mini-Q&A. “Does that mean it’s not the right thing to do? Absolutely not. Is pathology black and white? No. Do people want it to be? Yes.”
He’s also heard positive response from his clinical colleagues. “One endocrinologist looked at me and said, ‘Oh, thank God you’re doing this.’” So far, he says, he’s encountered very little confusion among his endocrine surgeons or endocrinologists. “They all recognize what we are trying to do and have supported it.” It’s likely more confusing to patients, he says. “This is about as granular as you can get.” It’s a papillary carcinoma, now without the carcinoma label, and a follicular variant, and it’s noninvasive. But for physicians, “It’s a pretty simple concept.”
Some clinicians take it a step further. Not only is NIFTP simple to understand, they say, but it’s also somewhat simplistic. “It’s a tempest in a teapot,” says Dr. Doherty, who was not involved in the study. Assuming the entity is treated with lobectomy—which it has been for decades, he says—nothing much has changed. While he calls it a well-done study, one that helpfully confirms earlier data, it doesn’t necessarily solve a long-standing problem he and his colleagues have been grappling with. NIFTP may be causing ripples, but it’s hardly threatening to break the levees.
The change might even create a new (if temporary) problem.
Clinical colleagues have raised few questions, says Dr. LiVolsi, but when they do it’s been at the prompting of patients who’ve read The New York Times article. “They want their tumor from two years ago to be reviewed, which is totally inappropriate,” says Dr. LiVolsi, who points to the obvious: Two years ago, the entity and the name did not exist. Patients were treated at the time according to the standards of the time, she says. “I feel strongly that research results—that’s what these are—do not belong in a patient’s medical record. To go back on the basis of somebody reading something in The New York Times? That’s wrong.”

Dr. LiVolsi
As of early May, Dr. LiVolsi had received one request. “I have refused to revise the diagnosis, and I have refused to look back at the slides. That case was signed out in 2012. In 2012, that was the diagnosis.”
Dr. Doherty is equally emphatic. He and his colleagues at Boston have heard from several patients wondering if the “new” tumor applied to them. “It hasn’t,” he says.
“We don’t see any clinical reason to go back and tell patients that a group of people has suggested we change the name of a low-risk disease they already knew they had. It doesn’t change clinical management at all. Changing the name doesn’t change the follow-up,” says Dr. Doherty.
Four years ago, Dr. LiVolsi notes, it was not the standard to examine the entire capsule. Older literature called for examining 10 sections of a nodule. “So you can’t apply current criteria or terminology to [a case from] two, four, six, 10 years ago and expect to bless it with this term.” It would, she agrees, be a bit like judging America’s founding fathers by today’s current moral standards.
Dr. Maytal, the MGH psychiatrist, also argues against such historical revisionism. “You operate with the knowledge that you had. At the time, they were given a diagnosis of cancer, and that’s what they had. That doesn’t negate or diminish anything they’ve experienced or however they were treated.”
These aren’t idle concerns. One pathologist has already heard from patients who are convinced their past lesions were misdiagnoses, and that they were overtreated as a result. But, says Dr. Nikiforov, “It’s important to stress that this was not an error before. This is a change in criteria; it’s not fixing an error.” The criteria, he reiterates, include examining the entire capsule, which might not be possible with archival cases.
Dr. Nikiforov mused on the possibility of revisiting old cases at the end of The New York Times piece. While he doesn’t say he misspoke to the reporter, he notes that when he and his colleagues then looked into doing it at UPMC, it quickly became clear how difficult the task would be. Not only might samples be insufficient for review, but would it be possible to contact former patients and their physicians? Rather than inviting such confusion, he and his UPMC colleagues are revisiting cases only at patient and/or clinician request, with results reported as an addendum rather than an amendment to the case.
Pointing the car in the other direction, so to speak, clinicians want firm answers about future cases. “They want to know how sure we are of the diagnosis,” Dr. Nikiforov says.
A NIFTP diagnosis is, in essence, a red traffic light. “They will stop completion thyroidectomy, they will stop radioactive iodine, they will stop very close follow-up,” Dr. Nikiforov says. “So they want to make sure pathologists are familiar with and understand how to make this diagnosis.”
Toward that end, in addition to reviewing cases as part of the study, Dr. Seethala, along with Dr. Nikiforov, oversaw development of the nuclear scoring scheme for including tumors into the NIFTP category.
“The scheme itself is not rocket science,” Dr. Seethala says. The basic nuclear features of PTC still form the basis for NIFTP, though the criteria have been restructured, Dr. Seethala says—the equivalent of moving furniture around rather than building a new house.
In the study, the scheme was used on still images of slides that were digitized in their entirety, to specifically focus on nuclear scores and increase reproducibility. In clinical practice, of course, pathologists will still need to find the relevant features themselves. “That’s going to be a challenge,” Dr. Seethala says.
There was some disagreement over the scores assigned to classify the nuclear features, Dr. Seethala continues. But collectively, within the test set and validation set, the accuracy was surprisingly high, based on prior review of the literature and given that reproducibility for nuclear features historically has been mediocre to poor, he says.
The scoring scheme should be useful in standardizing the NIFTP diagnosis, Dr. Seethala says, adding that its strength lies in how it was developed: The nine broad parameters used were assigned points, and a statistician reviewed the pathologists’ performances on both sets. “That type of thing is not typically done in pathology, despite its value,” he says. “It should be done more commonly,” he adds, though he admits it’s logistically difficult.
Though the published scheme should answer many questions, Dr. Seethala wants to make one point clear now: The grading scheme is not the only component of a NIFTP diagnosis. Its sole purpose is to help pathologists decide whether a tumor contains enough nuclear features to consider this entity.
Anticipating other misperceptions, Dr. Seethala pulls a few other potential weeds. “The general assumption is that this new category basically encompasses everything that we used to call encapsulated, well-demarcated or noninvasive follicular variant papillary thyroid carcinoma,” he says. “That’s true, to some extent.
“The difference is now we have a lot of criteria to ensure that we don’t keep in more aggressive tumors,” he continues. “As a result, you’re going to have to be stricter in terms of other growth patterns.” While they may have been a somewhat acceptable part of this category before, that’s no longer the case. This would include a true papillary component, solid component, and mitoses, which are now considered exclusionary criteria.
The goal, says Dr. Seethala, is to recognize that NIFTP is a neoplasm with a very low malignant potential based on the literature to date—nearly 500 cases. “But to ensure that, we have to keep this category fairly clean. That’s why the exclusionary criteria also come into play.”
At UPMC, Dr. Seethala says, the term NIFTP has already come into use. Because of the exclusionary criteria, “We’re finding we’re not using it as often as we anticipated.”
Reporting will continue to evolve, Dr. Seethala says. “If this is no longer equated at the same level as other carcinomas, AJCC staging is no longer relevant to this entity.” The relevant parameters are somewhat limited. “The name [NIFTP] implies the absence of a lot of things that we would normally report in a thyroid cancer in the CAP synoptic,” hence the current discussion about how/whether the synoptic should change. “Because it’s not entirely benign; it’s provisionally categorized into a very low malignant potential grouping. But it’s no longer ‘cancer.’” The CAP Cancer Committee’s head, neck, and endocrine panel is mulling it over, says Dr. Seethala, who is part of that group. “There may be room for a limited, optional data set,” he says. “The advantage of reporting these in synoptic form is that you can still capture these data points.”
Dr. Nikiforov sees two other long-term impacts, both of which he calls “quite interesting to think about.”
By way of background, thyroid cancer has been one of the fastest growing types of cancer in the United States as well as other countries, with rates tripling in the past 30 years. A significant portion, says Dr. Nikiforov, are what would now be called NIFTPs. Should this new category gain acceptance, it seems reasonable that the rate would drop, Dr. Nikiforov says.
More exciting, he says, is the possibility that this paper will point researchers in a similar direction for other indolent cancers, something the NCI has long been concerned about. The study could easily provide a blueprint for other groups that want to explore the possibility of reclassifying other types of indolent tumors. Indeed, he says he’s already been contacted by physicians who are interested in such work. “I hope this can have a profound effect, not only on pathology, but on the field of oncology.”
At its core, NIFTP is a surgical disease,but preoperative factors can predict its presence. The most potent are molecular markers.
The TCGA study (to simplify matters greatly) essentially identified two classes of tumors. It turns out, Dr. LiVolsi says, that the follicular variant of papillary carcinoma that is encapsulated—whether or not it’s invasive—tends to have molecular signatures closer to follicular adenoma than to classic papillary carcinoma. Although they share similar nuclei, from the molecular standpoint they really are not papillary carcinomas, says Dr. LiVolsi. “So these tumors not only appear to behave clinically very well, but also, at a deep level, they are different from papillary carcinomas.”
Dr. Nikiforov says he’s often asked if molecular testing is required to make a NIFTP diagnosis. His answer is simple: No.
Can the disease be predicted on molecular markers? His answer is just as succinct: Yes.
“The landscape of the molecular profile of NIFTP is pretty well defined,” Dr. Nikiforov says, as shown in the recent study and previous studies. “And now we are preparing another study to confirm it,” he says.
Four events—RAS mutations, PPARγ and THADA gene fusions, and (less commonly) BRAF K601E mutations (as opposed to the better-known BRAF V600E mutations)—are responsible for almost 90 percent of NIFTP. This gives rise to an interesting idea, Dr. Nikiforov says: Perhaps molecular testing on preoperative fine-needle aspiration biopsy can be used to make recommendations for lobectomy versus total thyroidectomy. UPMC routinely does such testing to reduce the extent of thyroidectomy, Dr. Carty says.
Another intriguing molecular development, says Dr. Nikiforov, is evidence that the more aggressive thyroid lesions have multiple mutations. If an examination of the nodule reveals only, say, a RAS mutation, there is a very good chance the tumor is a NIFTP, says Dr. Nikiforov. But finding RAS and, say, a TERT or TP53 mutation, “We know this is a really aggressive cancer and have to treat with total thyroidectomy.”
His UPMC colleague N. Paul Ohori, MD, professor of pathology, puts it in terms Ansel Adams would have appreciated: Molecular testing adds a layer of information to help sort out gray-zone diagnoses. “It’s adding or subtracting shades of gray,” says Dr. Ohori, medical director of cytopathology, UPMC Presbyterian.
Dr. Ohori’s main interest in NIFTP, not surprisingly, lies in implications for cytology.