Changes to practice expense result in overall decrease to pathology services
Charles Fiegl
December 2018—The CMS finalized its 2019 Medicare physician fee schedule and its response to the CAP’s recommendations to raise payment for fibrinolysins interpretation and reporting and to forgo a proposed decrease to the physician work value for blood smear interpretation.
{kind=link}
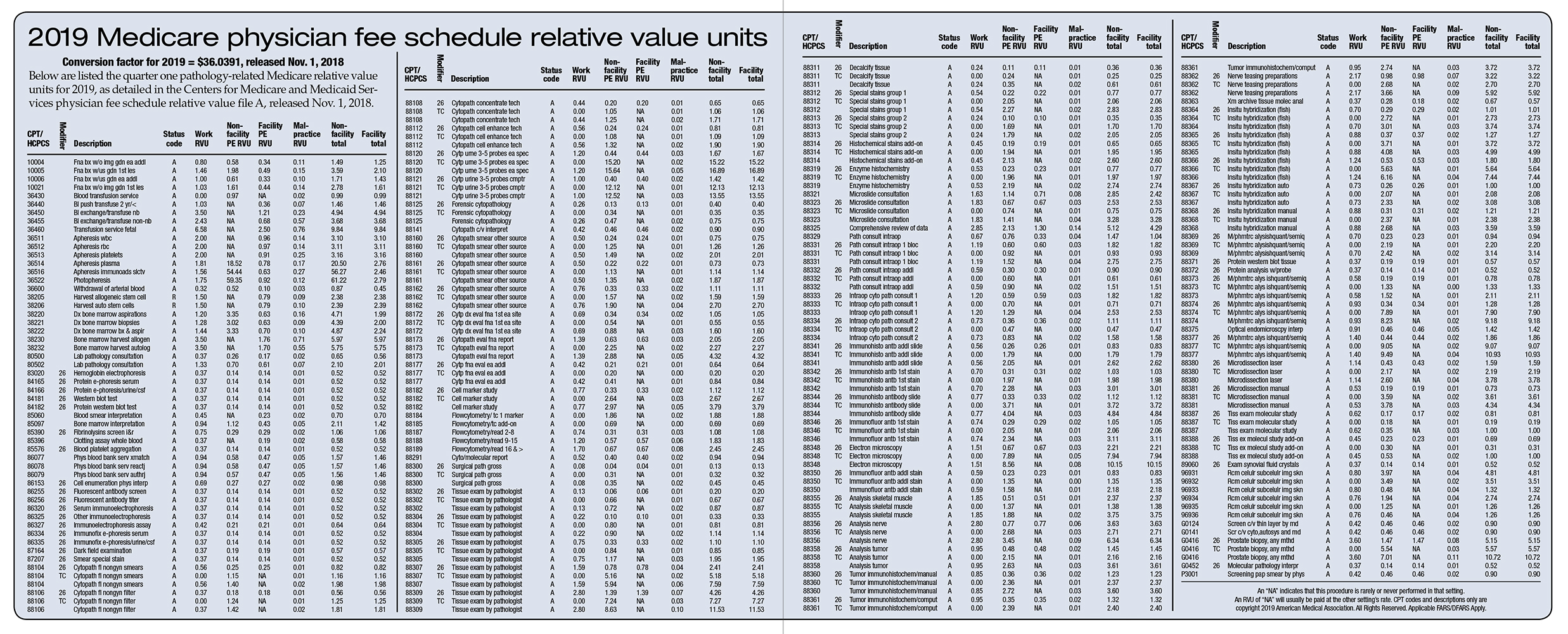
The Centers for Medicare and Medicaid Services on Nov. 1 published the 2019 physician fee schedule. Services on the physician fee schedule are composed of three relative value units designated by the CMS: physician work, practice expense, and malpractice liability RVUs. Each RVU is separately valued and summed to equal the total RVU for each physician service on the fee schedule. The CAP advocates for the appropriate valuation of pathology services through its representation on the advisory committee of the AMA/Specialty Society Relative Value Scale Update Committee, known as RUC.
A July 2017 Advances in Anatomic Pathology article, “Current valuation of pathology service,” coauthored by Jonathan L. Myles, MD, who served previously as the CAP’s member on the RUC advisory committee and serves now on the CAP Board of Governors, explains how pathology services are valued and notes that the work RVU component represents a “physician’s time to perform the service, the technical skill and physical effort, the required mental effort, and judgement, as well as the stress due to potential risk to the patient” (Myles JL, et al. 24[4]:222–225).
View 2019 Medicare physician fee schedule
After the proposed 2019 Medicare physician fee schedule was released in July, the CAP urged the CMS to accept the CAP-developed physician work RVUs that the RUC had approved and submitted to the CMS. In addition, the CAP developed direct practice expense inputs for pathology services, which are the basis of global payments as well as payment for the technical component.
Previously, the Medicare program had identified as potentially misvalued the service for fibrinolysins or coagulopathy screen interpretation and report (CPT code 85390), which triggered a review of its physician work RVU. The RUC reviewed it and recommended an increase in payment. The CMS agreed with the recommended value, and the service will be paid at the national rate of $38.20 in 2019, an increase of 104 percent from $18.72 in 2018.
The CMS also finalized 2019 payment changes for new and revised fine needle aspiration biopsy services. This CPT code family includes fine needle aspiration biopsy without imaging guidance (CPT codes 10021 and 10004), with ultrasound guidance (CPT codes 10005 and 10006), as well as FNA biopsy codes that include other imaging modalities. For FNA biopsy services (CPT codes 10021, 10004–10006), the CMS also agreed with most of the valuation recommendations from the CAP and its coalition partners after a review of new and revised codes for the services. After a thorough review, the RUC recommended a work RVU of 1.20 for CPT code 10021 (fine needle aspiration biopsy, without imaging guidance; first lesion), a slight decrease from the 2018 work RVU of 1.27. However, the CMS disagreed with the RUC-recommended work RVU for CPT code 10021 and finalized a work RVU of 1.03 based on a direct crosswalk to CPT code 36440 (push transfusion, blood, two years or younger).
The CMS accepted and finalized RUC recommendations for work RVUs of 0.80 and 1.00 for new CPT codes 10004 (fine needle aspiration biopsy, without imaging guidance; each additional lesion) and 10006 (fine needle aspiration biopsy, including ultrasound guidance; each additional lesion), respectively. The service 10005 (fine needle aspiration biopsy, including ultrasound guidance; first lesion) will have a 2019 work RVU of 1.46; the RUC had recommended a 1.63 work RVU.
The CMS agreed in the final fee schedule with the CAP recommendation to maintain payment for CPT code 85060. After the CMS had proposed a decrease in July, the CAP defended the developed value and urged the CMS to adopt the RUC approved value. A number of variables should be considered in the evaluation of a blood smear when compared to others, the CAP said in its comments, including red blood cell count, size and morphology, platelet morphology and number, white blood cell morphology, and the presence of WBC precursors. The CMS accepted the current work RVU of 0.45.
The CMS did not agree with the CAP and RUC recommendation to increase payment for CPT code 85097 (bone marrow, smear interpretation) by increasing the work RVU for the service to 1.00 from its 0.94 value for 2018. Instead, the CMS is maintaining the current work RVU of 0.94 for 2019.
Overall, the CMS projected that changes in the fee schedule will result in a two percent decrease in Medicare allowed charges to pathology services next year. The decrease is largely due to final changes to practice expense RVUs after an extensive review of supply and equipment prices. In the payment for physician services, the practice expense RVUs include the costs associated with nonphysician or clinical labor time in addition to the costs of the supplies and equipment used to furnish the service.
The last time the CMS systematically reviewed prices to develop practice expense RVUs was 2004–2005. The Protecting Access to Medicare Act of 2014 authorized the CMS to use other sources to determine RVUs. For the recent effort, the CMS contracted with the firm StrategyGen to submit a report with pricing recommendations for 1,300 supplies and 750 equipment items used for direct practice expense units. The CMS accepted the recommendations and, starting in 2019, is phasing in the practice expense inputs over a four-year period.
After the CMS released its proposed rule in July, the CAP reviewed the StrategyGen pricing recommendations and noticed a number of new prices that appeared to be inaccurate by not reflecting either the proper product, quantity, or unit of measure for the service. Concerned about the accuracy of the prices, the CAP urged the CMS to postpone implementing StrategyGen’s recommendations so physician specialties can review and provide further comment on the inputs affecting practice expense RVUs. In response to the CAP’s concern and those of other physician specialty associations, the CMS disagreed that delaying implementation of the pricing inputs would lead to more accurate pricing. However, the CMS encouraged physicians to identify supply and equipment codes that will require additional research throughout the four-year transition. Additional information provided by the CAP to the CMS may result in updates to inputs to supply and equipment items. The CAP is working with the agency on prices for supplies that pathologists and laboratories use by, for example, submitting invoices for equipment.
In advocating for appropriate valuation, the CAP gathers information through the RUC’s physician work survey process. The surveys collect information about each of the components of physician work and provide for a comparison of that work with other pathology services and with other specialties’ services to develop a physician work RVU recommendation. The CAP’s RUC advisor presents the RUC survey data and recommendations to the RUC for consideration. The RUC submits its recommended values and other data to the CMS for use in the proposed physician fee schedule. The CMS can accept the recommendation, alter it, or reject it and value the service using its own analysis. The CAP advocates for adoption of the CAP-developed values in the final Medicare physician fee schedule.
Charles Fiegl is director of CAP advocacy communications, Washington, DC.