
Anne Ford
March 2018—When it comes to diagnostic tests, everyone wants the same thing Lars Westblade, PhD, wants: A unicorn.
“The diagnostic performance of a test is reflected in its sensitivity and specificity,” Dr. Westblade said. “It has to be a very good test. And then we need to think about the speed of the test.” There’s also the cost. When all these factors come together just so, “we get what’s called diagnostic perfection,” he says, or the rare event that Brandi Limbago, PhD, of the CDC calls “a diagnostic unicorn.”
When it comes to diagnostic tests, everyone wants the same thing Lars Westblade, PhD, wants: A unicorn.

“The diagnostic performance of a test is reflected in its sensitivity and specificity,” Dr. Westblade said. “It has to be a very good test. And then we need to think about the speed of the test.” There’s also the cost. When all these factors come together just so, “we get what’s called diagnostic perfection,” he says, or the rare event that Brandi Limbago, PhD, of the CDC calls “a diagnostic unicorn.”
Mythical creatures, diagnostic or otherwise, are in short supply. Unfortunately, multidrug-resistant organisms are not.
Dr. Westblade is an assistant professor of pathology and laboratory medicine at Weill Cornell Medicine and associate director of clinical microbiology at NewYork-Presbyterian/Weill Cornell Medical Center. In a webinar hosted by CAP TODAY and made possible by an educational grant from Cepheid, he walked laboratories through the tests that detect one of the most dangerous groups of multidrug-resistant organisms: carbapenemase-producing carbapenem-resistant Enterobacteriaceae (CP-CRE). (His co-presenter, Stephen Brecher, PhD, spoke on CP-CRE, β-lactamases, and antibiotic breakpoints. See page 12.) Dr. Westblade also spoke with CAP TODAY recently.
“Our physician colleagues would like to know their patient had a CP-CRE sooner rather than later,” he said. They’ll likely treat it more aggressively, and there are antimicrobial agents (e.g. ceftazidime-avibactam, imipenem-relebactam) available that are selective for certain classes of carbapenemase. These agents could be administered almost immediately when a particular carbapenemase is identified.
When using a carbapenemase detection test for routine intra- or inter-facility infection control, the test needs to reveal the presence or absence of a carbapenemase, and perhaps also differentiate between classes. “Do we really need to know if it’s a serine- or metal-based enzyme?” Dr. Westblade asked. “I’m not quite sure. But if we can get that information, why not?”
 “Certainly in the setting of an outbreak,” he added, “differentiation of carbapenemases would be very useful to allow identification of related cases.”
“Certainly in the setting of an outbreak,” he added, “differentiation of carbapenemases would be very useful to allow identification of related cases.”
For public health surveillance, a carbapenemase detection test needs to be very specific, “because we’re now at the point of confirming and identifying the exact mechanism of carbapenemase activity,” Dr. Westblade said. “We want to get to the nitty-gritty.”
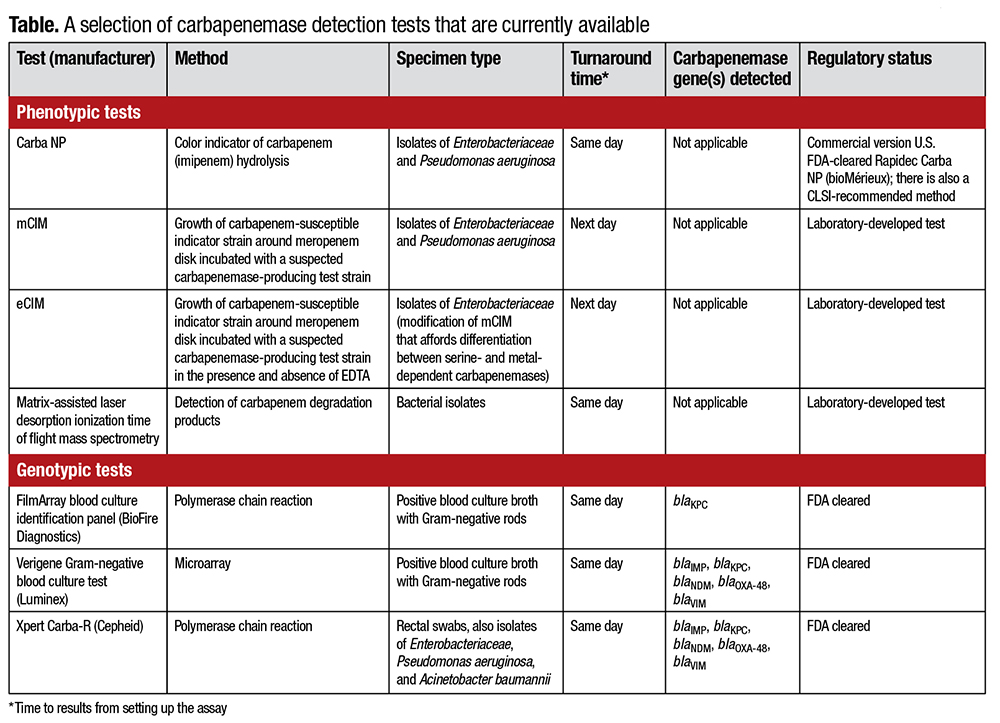
CP-CRE can be detected directly from clinical specimens (positive blood cultures or rectal swabs) or in bacterial isolates recovered in culture using genotypic or phenotypic assays (Table, page 19). Identifying these isolates in clinical specimens is achieved using PCR or microarray tests, while several assays, genotypic and phenotypic, can detect the presence of a CP-CRE recovered in culture.
Of the genotypic carbapenemase detection tests, Dr. Westblade said, “We get results the first day, really within two hours, that the specimen arrives in the lab or a blood culture broth becomes positive. But they’re expensive, certainly compared to phenotypic assays and other tests traditionally associated with the microbiology lab. However, they have the potential to reduce downstream costs and, most importantly, save patient lives. We need to move past the silo mentality.”
Phenotypic carbapenemase tests for use with CP-CRE obtained in culture include the modified Hodge test. “We take a carbapenem-susceptible indicator strain, apply it to the surface of a Mueller-Hinton agar plate, and then place a disk impregnated with a carbapenem on the plate. Subsequently, we streak a suspected CP-CRE test isolate from the edge of the paper disk to the edge of the agar plate,” Dr. Westblade explained. It is then incubated overnight at 35° C. “We’re looking for invagination of the zone of growth inhibition of the indicator strain—that carbapenem-susceptible strain—around the test isolate. This is considered a positive result.”
While the modified Hodge test has, for most carbapenemases, good sensitivity, it also produces notable false-negative and -positive results. As of this year, the Clinical and Laboratory Standards Institute no longer recommends this assay. In other words: “Dodge the Hodge.”
Another phenotypic carbapenemase detection test is the modified carbapenem inactivation method (mCIM). In this assay, “we re-suspend a CP-CRE test strain in 2 mL of tryptic soy broth with a 1 µL loop,” he said. “We throw in a meropenem disk and incubate the test strain with the meropenem disk for four hours at 35° C.” After this incubation period, the meropenem disk is placed on a Mueller-Hinton agar plate inoculated with a carbapenem-susceptible indicator strain. “If the test isolate is not a CP-CRE, we’ll see a zone of growth inhibition”—meaning that the meropenem in the disk was not hydrolyzed by the test isolate and is still capable of inhibiting the growth of the carbapenem-susceptible indicator strain. Conversely, if the test strain is a CP-CRE, the meropenem in the disk will be hydrolyzed, rendering it inactive. The carbapenemase-susceptible indicator strain can grow right up to the meropenem disk.
Dr. Westblade calls it “a very clever test,” pointing to a multicenter evaluation of the assay showing that it performs very well with the different classes of carbapenemases: A, B, and D enzymes. The CLSI now recommends it for use with Enterobacteriaceae. This year, Pseudomonas aeruginosa will be included as well.
A variation of this test, the EDTA-modified carbapenem inactivation method (eCIM), affords the differentiation of serine and metallo-β-lactamases. EDTA is an inhibitor of metallo-β-lactamases. “This test could be important for making therapeutic decisions and also allow an institution to have a higher understanding of its epidemiology,” Dr. Westblade said. Both the mCIM and eCIM use readily available off-the-shelf reagents and can be implemented in “pretty much any laboratory in the world.” “But you only interpret the eCIM result if the test isolate produces a carbapenemase as determined using the mCIM,” Dr. Westblade said.
Another phenotypic carbapenemase detection test, Carba NP, takes advantage of something that happens when a carbapenemase hydrolyzes a carbapenem: a change in pH. The creators of the assay, “brilliantly I might add, thought, ‘Why don’t we exploit this change in pH to develop a test,’” Dr. Westblade said. “When we mix extracts of a test isolate devoid of carbapenemase activity with a pH indicator and a carbapenem, there is no pH change. But if you’ve got a CP-CRE, the carbapenem is hydrolyzed, causing a change in pH, which is registered by the pH indicator.”
A multicenter evaluation of the Carba NP assay revealed what Dr. Westblade called “okay” sensitivity and specificity, with sensitivity of around 70 to 90 percent and specificity between 93 and 100 percent. “It was noted to have poor performance with those tricky OXA-48-like enzymes we can find in Escherichia coli and Klebsiella pneumoniae.” In the CLSI-recommended method described in the M100 document, some of the reagents are prepared fresh, which “could be a little bit limiting for labs,” he noted. However, there is an FDA-cleared commercial version, the Rapidec Carba NP, which simplifies the process. The CLSI recommends this test for detection of carbapenemase activity in isolates of Enterobacteriaceae and Pseudomonas aeruginosa.
One advantage of genotypic-based tests is that they allow the precise identification of the gene encoding the carbapenemase. Rapid results can be obtained with clinical specimens and bacterial isolates. “Purity is not necessary. They’re agnostic of purity,” Dr. Westblade said. Furthermore, “they can be multiplexed. Multiple carbapenemase genes can be probed simultaneously.”
However, there are disadvantages. Multiplex assays only detect certain carbapenemase genes. “So if you have a new enzyme variant, or an uncommon enzyme that’s not included in your multiplex panel, it can be missed, whereas a phenotypic assay detects activity and is probably not going to miss the presence of a carbapenemase.” Furthermore, the presence of a gene is not always associated with resistance. “It may not be expressed.” And these assays are generally expensive compared with phenotypic assays.
To the best of Dr. Westblade’s knowledge, there are three FDA-cleared genotypic platforms on the market. Two of them, the FilmArray blood culture identification panel and the Verigene blood culture Gram-negative panel, are for use with positive blood cultures. The FilmArray test detects the gene encoding the KPC enzyme. The Verigene assay probes for the genes encoding IMP, KPC, NDM, OXA-48, and VIM enzymes.
The third test, the Xpert Carba-R assay, is FDA cleared for rectal swab specimens and Enterobacteriaceae, Pseudomonas aeruginosa, and Acinetobacter baumannii isolates recovered in culture. This PCR-based assay identifies the genes encoding IMP, KPC, NDM, OXA-48, and VIM enzymes. A multicenter study found that it performed very well with rectal swab specimens, displaying a sensitivity of 97 percent and specificity of 99 percent. “It, like the other genotypic tests, does require some infrastructure,” Dr. Westblade noted, referring to the need for dedicated instrumentation to run these assays.
One final way of detecting carbapenemase genes employs “a technology that I’m in love with,” he said. “It’s the application of next-generation DNA sequencing methods to sequence bacterial chromosomal and extrachromosomal DNA either isolated from the bacterium itself or within clinical material.” Of the several next-generation DNA sequencing platforms available, his favorite is the MinION platform from Oxford Nanopore Technologies. “I love this system because it’s about the size of an iPhone, is extremely portable, having been employed for Ebola real-time surveillance in the field, and sequences DNA by threading it through a membrane protein. Now if that isn’t X-Files or Star Trek, I don’t know what is,” he said.
Next-generation DNA sequencing assays should be able to detect all currently known carbapenemase genes, Dr. Westblade said. “And they also provide additional information. They’re an open-ended test. We can determine strain relatedness, so we can use them to track transmission events. And we can even detect other resistance determinants. Some labs have started to use these systems to generate so-called virtual antimicrobial susceptibility testing results.”
He presented what he called a “beautiful” example from the NIH Clinical Center, in which a patient who was known to harbor a KPC-producing Klebsiella pneumoniae isolate was hospitalized in June 2011 and discharged the following month. In August of that same year, a second patient was positive for a KPC-producing K. pneumoniae. It was found that, on average, one new KPC-producing isolate was isolated each week, for a total of 17 cases, until the outbreak was stopped the following January.
“And because Klebsiella pneumoniae is highly clonal in the United States, with 70 percent of KPC-producing Klebsiella pneumoniae belonging to one sequence type, ST-258, conventional typing platforms weren’t useful in this setting,” Dr. Westblade said. “Deciphering the transmission events between these patients based solely on epidemiologic data was impossible.” Specifically, the epidemiologic data could not discriminate between undetected transmission from the index patient or introduction of a second strain.
“They took multiple isolates from the index patient cultured from different anatomic sites, which was genius, and also a single isolate from each of the 17 cases and submitted them for whole-genome sequencing using next-generation DNA sequencing methods.” Based on these data, together with epidemiologic information, the investigators were able to identify direct linkage with the index patient, with transmission originating from different anatomic sites.
Ultimately, Dr. Westblade concludes, an institution’s local epidemiology will dictate the necessity, method, and frequency of testing for CP-CRE, and other carbapenemase-producing organisms.
“However, I encourage all labs to have readily available access to some form of carbapenemase detection test,” he said, “and to work closely with infectious diseases, infection control and prevention, and antimicrobial stewardship specialists within their institution to manage infections due to these organisms and to prevent their spread.”
[hr]
Anne Ford is a writer in Evanston, Ill. The full webinar is available at www.captodayonline.com.