Karen Lusky
June 2021—A case of monoclonal B-cell lymphocytosis and a tour of B- and T-cell morphologies were at the heart of a CAP20 virtual presentation on neoplastic lymphocytosis.
Kyle Bradley, MD, associate professor of hematopathology and director of surgical pathology at Emory University, spoke last fall on reactive (CAP TODAY, May 2021) and neoplastic lymphocytosis, with Olga Pozdnyakova, MD, PhD, who addressed neutrophilia and monocytosis (CAP TODAY, February and March 2021). Together they took attendees through a morphology-based approach to hematopoietic neoplasms presenting with an abnormal WBC differential.
“Some malignant lymphocytes can closely resemble normal cells,” Dr. Bradley said in a recent interview. “The classic example would be chronic lymphocytic leukemia because individual lymphocytes in that neoplasm can look very similar to normal lymphocytes.”
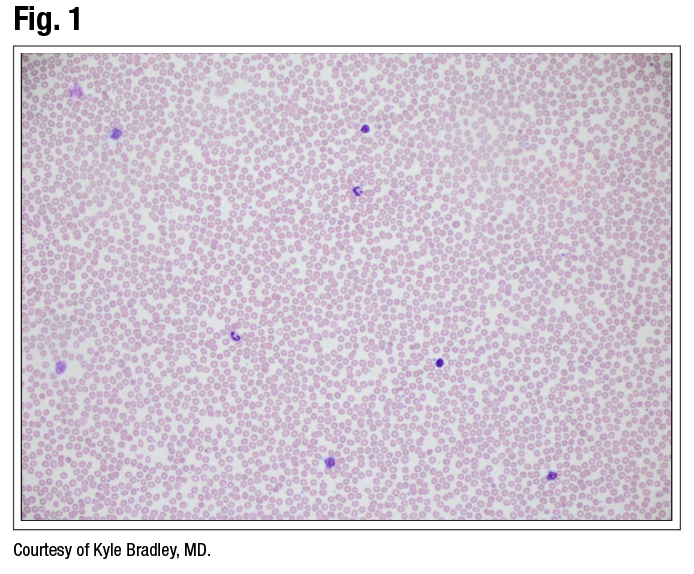
Dr. Bradley shared the case of a 59-year-old man with a clonal B-cell population identified by flow cytometry. It was positive for CD19, CD20, CD5, CD23, CD200, and Kappa, and negative for CD10, FMC7, and Lambda. “This is a typical phenotype for chronic lymphocytic leukemia/small lymphocytic lymphoma,” he said. However, “the blood smear is not what you typically think of for CLL.” (Fig. 1).
{kind=link}
The differential diagnosis is CLL versus monoclonal B-cell lymphocytosis, he said. In the current and previous WHO classification, CLL requires greater than 5.0 × 109/L clonal B cells. Lower counts are acceptable if there are signs or symptoms of lymphoma. Monoclonal B-cell lymphocytosis is defined as ≤ 5.0 × 109/L clonal B cells in otherwise healthy subjects. “So this means we have to figure out what the clonal B cell count is with our patient.”
In talking to the clinician or studying the medical record, he and colleagues find the patient is healthy, with no lymphadenopathy. The white blood cell count is 10.9 × 109/L. “We can go back to the flow and figure out what percent is the B-cell clonal population.” The clonal B cells, they find, are 36 percent of all white blood cells. “So 36 percent of 10.9 gives you an absolute count of 3.9 × 109/L. This is less than or equal to five. It’s a healthy patient. So this is indeed monoclonal B-cell lymphocytosis,” Dr. Bradley said, noting that MBL is now known to precede essentially all cases of CLL. “You can think of this the same way you think about MGUS [monoclonal gammopathy of undetermined significance] progressing to myeloma where we know this is a precursor condition that requires some follow-up.”
MBL has three phenotypes. The first and most common is CLL-like (about three-fourths of cases). The second, atypical CLL phenotype, is CD5 positive like CLL, but it has other atypical phenotypic features. “Maybe CD23 is dim or negative, which is not typical,” Dr. Bradley said, “or maybe CD20 is brighter than you’d expect for CLL.” To rule out mantle cell lymphoma in these cases, he said, FISH is recommended to look for t(11;14) IGH-CCND1. If the patient has mantle cell lymphoma, “there is no MBL version of mantle cell lymphoma. So if you diagnose even a small population of mantle cell, it’s mantle cell,” he said, “and that’s how you should diagnose it.”
The third phenotype is non-CLL, which is any that are clonal and CD5 negative. “We know these are closely related to splenic marginal zone lymphoma.”
The bone marrow is typically involved in monoclonal B-cell lymphocytosis. “The median percentage of clonal B cells in the marrow is 20 to 30 percent, but I’ve seen cases where it’s more than half of the marrow,” Dr. Bradley said. There are no bone marrow criteria for differentiating CLL from MBL.
If a bone marrow is half full of CLL cells by flow cytometry, and “you don’t know the white blood cell count and cannot distinguish between MBL and CLL,” he said, “you should not call this marrow CLL.” He said he sees that done often and considers it incorrect. “I’ll diagnose it as marrow involvement by a clonal B-cell population.” Often he can figure out the white count or he knows the clinical history and can determine if the patient has lymphadenopathy.
New in the 2017 WHO classification is the separation of low-count (< 0.5 × 109/L, median 0.008 × 109/L) from high-count (0.5–5.0 × 109/L, median 3.38 × 109/L) CLL-like MBL. Dr. Bradley said the primary reason low-count CLL-like MBL are separated out is that they have no significance clinically. “These are found with generally sensitive flow techniques and have not been shown to progress and don’t require follow-up.” High-count CLL-like MBL needs annual follow-up. One to two percent per year progress to CLL, comparable to MGUS progressing to myeloma.
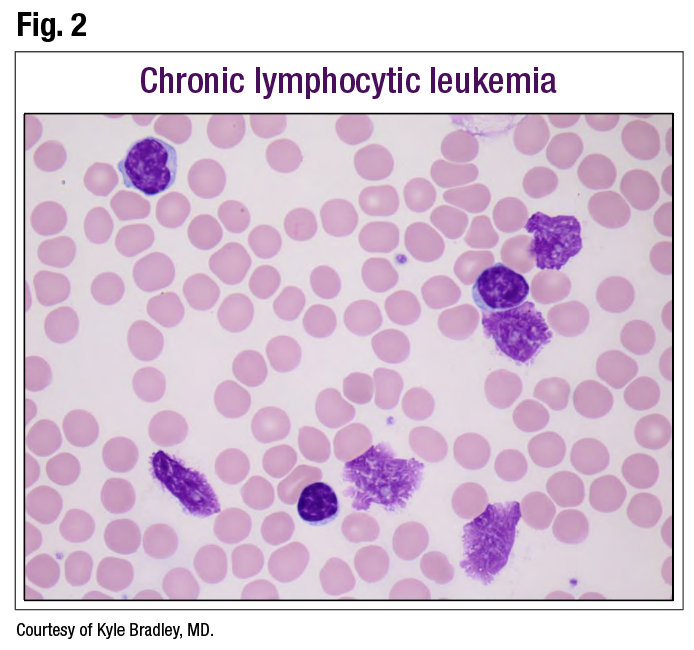
Dr. Bradley presented several B- and T-cell neoplasms, starting with classic CLL (Fig. 2), which has small lymphocytes. Smudge cells in the background are characteristic, “but don’t equate smudge cells with CLL. That’s not specific enough,” he said.
{kind=link}
In these cases, the chromatin has characteristic features: “cracks or little linear areas, so-called soccer ball chromatin or cracked earth,” he said. In most cases of CLL, “any individual lymphocyte you look at is difficult to distinguish from a normal lymphocyte.” Flow cytometry is the first step.
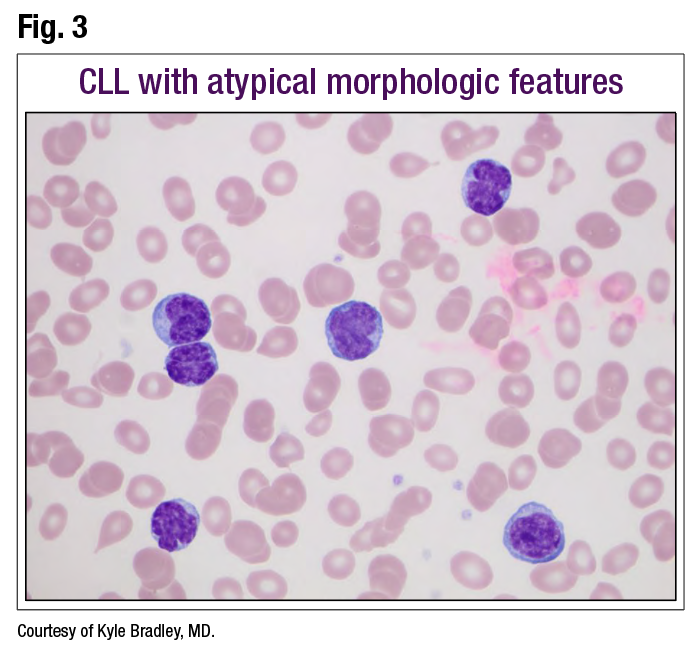
Some CLL cases will have more atypical morphologic features (Fig. 3). “It’s sort of monotonous, and lymphocytes are not normal, so flow cytometry is indicated. If you do flow and get your classic CLL phenotype, then this is just CLL. You don’t need to make more of it.” With atypical morphology, there may be prognostic differences, he said, but FISH or immunoglobulin variable region gene studies and other methods are used to further assess prognosis in CLL.
{kind=link}
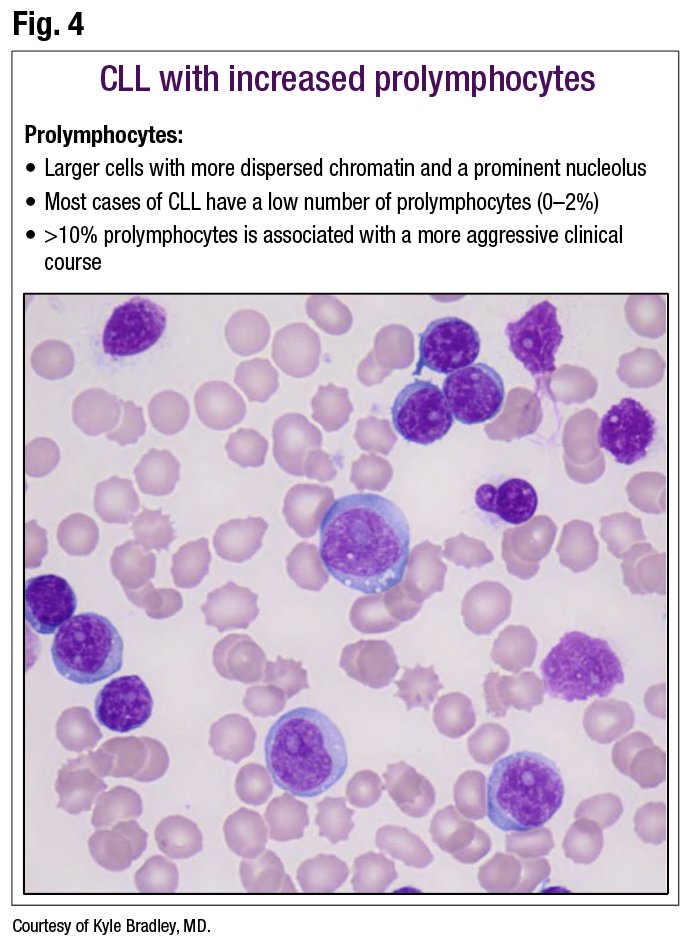
Each time Dr. Bradley sees a CLL case, he said, he assesses it for the number of prolymphocytes and he recommends that others do the same. In (Fig. 4), the typical prolymphocytes are present, mixed in a background of CLL with smudge cells. The reason to identify these, he said, is that most cases of CLL will have very low numbers of prolymphocytes. “In some cases, you won’t find any or it’s hard to find even one. In some cases you may have one or two percent. That’s typical for CLL and doesn’t warrant any additional worry to impart to the clinicians, but I do put it in my report” for the purpose of a lookback.
{kind=link}
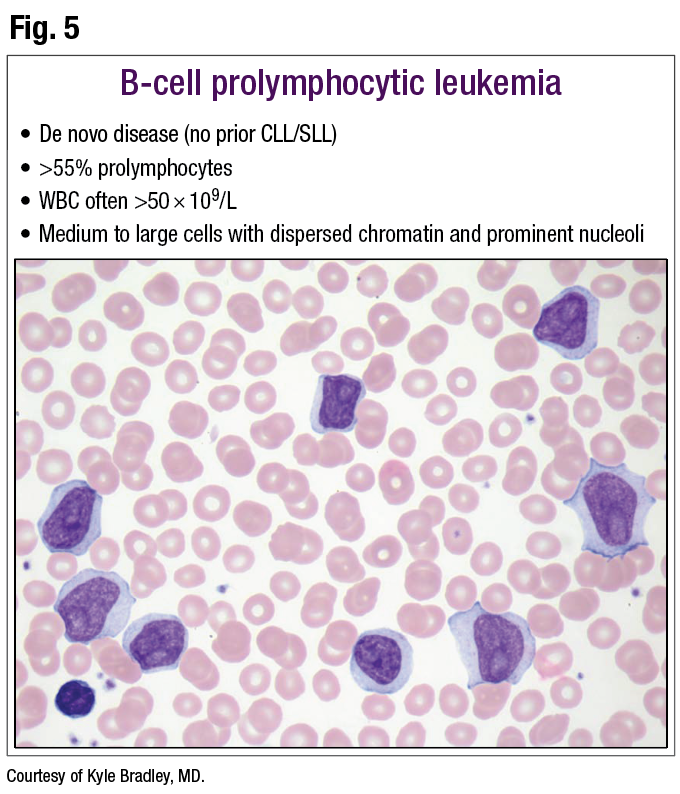
B-cell prolymphocytic leukemia (Fig. 5) is a neoplasm for which medium to large cells with dispersed chromatin and prominent nucleoli are characteristic. Diagnosis of B-PLL has to be a de novo disease, Dr. Bradley said—no history of CLL or small lymphocytic lymphoma. If the patient has a history of CLL and the pathologist sees something like this, he said, the correct diagnosis would be prolymphocytic transformation of CLL.
{kind=link}
B-PLL is defined as greater than 55 percent prolymphocytes. “The white count is classically very elevated, often greater than 50,” he said. Flow cytometry is the next step.
Hairy cell leukemia is the classic one for morphology (Fig. 6). In his experience, he said, “hairy cell leukemia is a lot less exciting on a blood smear than the book images lead you to believe.”
{kind=link}
“When I was first learning this, I saw the beautiful images of the big hair-like projections.” When he started to see cases, he said, “it was hard to find cells that have those wonderful projections.”
It’s more common to see “a ruffled or frilly kind of border to the cytoplasm,” he said, adding that paying attention to the nuclear features is important. “I know the cytoplasm and hair-like projections get all the press, but the nuclear features are also somewhat distinctive in hairy cell. The nuclei are generally oval, or may be kidney-bean shaped, and eccentrically placed, because there is some moderate amount of cytoplasm.”
Patients are frequently cytopenic in hairy cell leukemia, Dr. Bradley said, and usually the abnormal cells are “few and far between. There’s not that many of them because there’s pancytopenia, including lymphopenia.”
Monocytopenia is a characteristic feature. “So if you can’t find a monocyte, or a very low zero to one percent monocytes, that’s typical for hairy cell leukemia, and relatively specific among lymphoid malignancies in the blood. Splenomegaly is typical, and essentially every case will have a BRAF V600E mutation.”
Hairy cell leukemia variant (Fig. 7) is not a variant of hairy cell leukemia, “but it does share some features, which is why it originally got that name,” Dr. Bradley said. “If I see something that looks like hairy prolymphocytes, that’s likely hairy cell leukemia variant.”
{kind=link}
He explains: “They have prolymphocyte-like nuclei with prominent nucleoli. These are not a feature of typical hairy cell leukemia, but then the cytoplasm has features that are typical for hairy cell leukemia with that ruffled and hair-like projection.”
Other features of hairy cell leukemia variant are a usually normal monocyte count, a significant increase in the white count, absence of the BRAF V600E mutation, and the possible presence of MAP2K1 mutations. Biologically, hairy cell leukemia variant is unrelated to HCL. “They share some phenotypic characteristics and some morphological characteristics,” he said, “which is why it has the name it has.”
For follicular lymphoma (Fig. 8), pathologists usually get a staging bone marrow, and while the marrow is ordinarily involved, blood involvement is rare. The centrocyte morphology is small to medium-size cells with a nuclear cleft. “And these will have the translocation (14;18) IGH-BCL2 in most cases.”
{kind=link}
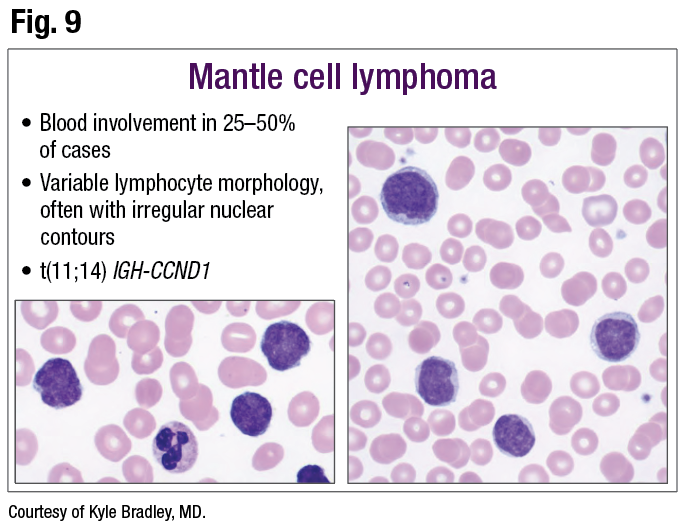
Blood involvement is more common (25 to 50 percent of cases) in mantle cell lymphoma (Fig. 9), but the lymphocyte morphology is variable, often with irregular nuclear contours. The translocation (11;14) IGH-CCND1 can be evaluated to help make the diagnosis, he said.
{kind=link}
Dr. Bradley turned to T-cell neoplasms with interesting morphologic features, the first of which is T-cell prolymphocytic leukemia (Fig. 10). “The characteristic feature is cytoplasmic blebs. Very distinctive, though sometimes they’re more subtle.”
{kind=link}
“You may see some nucleoli. They do have a name of prolymphocyte, but it’s variable how much you’ll see the nucleoli,” he said, urging pathologists to consider T-cell prolymphocytic leukemia when they see cytoplasmic blebs and a T-cell phenotype. “The white count in these cases is usually markedly elevated, often greater than 100. A 300 or 400 white count is not uncommon at all in T-PLL.” To help solidify the diagnosis: “Recognize that on chromosomes, about 80 percent of cases will have an inversion 14, and that’s relatively specific for this diagnosis,” Dr. Bradley said.
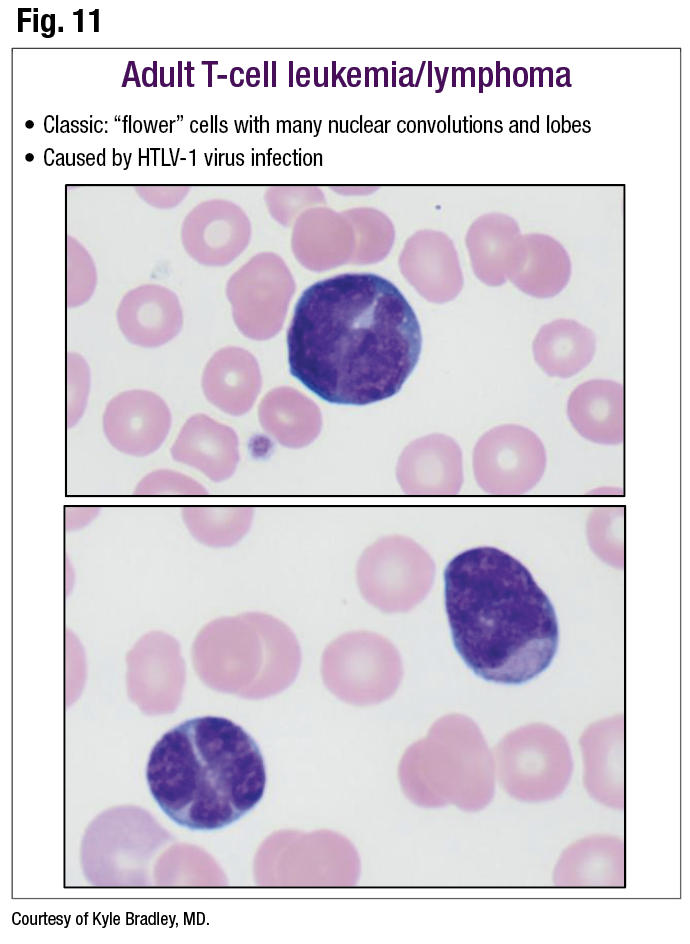
The classic finding in adult T-cell leukemia/lymphoma, or ATLL (Fig. 11), is flower cells, which are cells with flower-like nuclei with many nuclear convolutions and lobes (lower box, cell on left). “This is one where you would want your clinicians to do HTLV-1 virus testing by serology,” he said, “because there is a very high association between that virus leading to this disease.”
{kind=link}
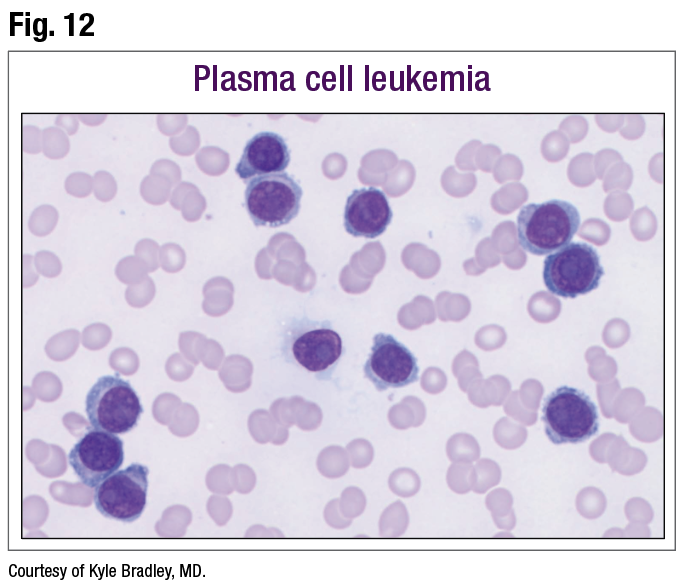
Last is plasma cell leukemia (Fig. 12). “There are some things to be aware of when you’re evaluating smears and suspicious for plasma cell leukemia,” Dr. Bradley said. Fig. 12 is a typical case: “There’s probably anemia, and there is a high lymphocyte or plasma cell count in this case, with lymphoid or lymphoplasmacytic cells,” some of which have typical plasma cell features. “Yet there are no beautiful classic plasma cells like you see in tissue or in bone marrow aspirates.”
{kind=link}
“The plasma cells will look much more lymphocyte-like and much less impressive.” (Fig. 13). Pathologists need to be aware of that, he said, because if they are asked to evaluate for plasma cell leukemia and look for typical plasma cells, they won’t find them in most cases.
{kind=link}
Karen Lusky is a writer in Brentwood, Tenn.