
Charna Albert
August 2023—With patient access to pathology reports now common via online portals, the question some have asked is what can be done to make them easier for patients to understand.
“They have access to the report. They are reading their report,” says Jason Wasserman, MD, PhD, assistant professor at the University of Ottawa and a head and neck pathologist at Ottawa Hospital. He asks: “Do we want patients to read them and to understand them? Or do we want patients to read them and misunderstand them and then go into their appointment with the wrong information, ill-prepared to talk about their condition?”
To Dr. Wasserman, the answer was clear six years ago when he was a fellow at University Health Network in Toronto and patients were beginning to have access to their reports through the online portal. In a conversation with a colleague, he recalls saying, “Someone should make a website that explains pathology to patients.”
“The idea was just, let’s throw up a couple of definitions to see if we can help patients understand,” he says.
Those definitions now number more than 500. And the website he built and where they can be found (mypathologyreport.ca) offers far more.
Today, at Ottawa Hospital and “thousands of hours” later, Dr. Wasserman sees to it that the website he launched in 2017 while at UHN consists of easy-to-understand articles on more than 500 of the most common pathology diagnoses and a dictionary of common pathology terms and phrases. Also on the site: answers to frequently asked questions, an atlas of images, and a function that makes it possible for patients to “Ask a Pathologist” a question.

Dr. Wasserman and 10 pathologist volunteers write the site’s content, which seven patient advisors review. (More than 25 others have contributed articles.) The diagnostic articles encompass all body sites and a variety of malignant, benign, and non-neoplastic conditions. Each article begins with a brief explanation of the normal anatomy and histology of the organ system involved, followed by sections explaining the standardized reporting elements (Lafreniere A, et al. J Clin Pathol. 2020;73[8]:454–455). Some also include simplified diagrams of normal and abnormal features, illustrated by Zuzanna Gorski, MD, a pathology resident at Ottawa Hospital. The team typically adds two articles each week.
“Everything we do is original content,” Dr. Wasserman says. “We’re writing an article from scratch and answering questions we think would be helpful to patients, so it does take time.” A hosting company handles the site’s backend management; Dr. Wasserman handles site administration. “I put the original website together, and I continue to upload the articles,” he says. “It’s a pathologist all-in endeavor.”
Initially, Dr. Wasserman struggled to figure out how to describe pathology in ways that patients could understand. “That was the biggest challenge,” he says. “How I was going to say these things and get around the barriers in my mind of what I knew as a gestalt looking in the microscope, but what I couldn’t put into words.”
Though he tried to focus on what he thought patients would want to know, “with hindsight, I realized what I did was talk about what I as a pathologist think is interesting about these words, about these diagnoses—what I as a pathologist would want a patient to know.” With the help of the patient advisors from Ottawa Hospital and UHN, “I realized there was information that didn’t need to be there,” he says, such as detailed explanations of the pathological features, but there also were missing elements, like why certain terms might appear in a report and why they were significant for the patient’s care. With the advisors’ guidance, he and his team also began to write in a question-and-answer format. One such question: “What is the Nottingham histologic grade for invasive ductal carcinoma with apocrine features and why is it important?”
“We try to focus on those kinds of things because that’s what patients wanted to know,” Dr. Wasserman continues. “My report says it, but why does it matter to me, and what should I be thinking of when I read this?” The patient advisors help pose the questions, he says. “We show them our articles in draft form, and they say, ‘What about this—why is this important to us?’”
Ottawa Hospital and UHN have embedded the site in the electronic health record, allowing patients to access it directly from the online patient portal, and other hospitals in Canada and the U.S. have added a link to their portals. “Because the site is freely accessible, people don’t have to tell us they’re putting in a link. They just do it. We want it to be as accessible to everyone as we can make it, so we’d like to see hospitals and labs all over the world putting a link in so people can find it,” Dr. Wasserman says.
Google has been the biggest source of traffic to the website. “A lot of patient support groups are talking about it,” he says. For the most part, “it’s word of mouth.”
The Ottawa Hospital has put up fliers in patient waiting areas, which helps reach patients less likely to use the online portal. “Certain groups are more able to access those things when left to their own devices, whereas everyone comes to the clinic to see their doctor,” he says. “If you make those resources available right where they are, you’re likely to flatten out some of those disparities.”
Dr. Wasserman’s goal for the website is to have the top 90 percent of all diagnoses from each body site represented. “Pathologists often make the same diagnosis over and over again,” he says, “so a small number of diagnoses capture a large number of reports,” and with the top 90 percent represented, most patients who visit the site will be able to find an article that helps them. He and his team also are working on a series of videos to help patients better understand the diagnostic process. “We often get questions from patients about the process: what happens in their biopsy, what’s going on behind the scenes, why is it taking a while for this [result] to come out, what was the pathologist looking at when they made this diagnosis.” Also in the plans are longitudinal studies comparing how patients read reports on their own versus reading reports with the aid of the site.
In the “Ask a Pathologist” section of the site, patients submit questions about their own pathology reports, and the pathologist volunteers answer those emails. “It was strange for me, the first couple times I answered emails,” Dr. Wasserman admits. “To get a question from a patient saying, ‘This is what my report says; what does this mean? What does this test result say about my condition?’ I wasn’t used to providing answers directly to a patient.”
“But I think this is something pathologists should be able to do,” he adds. “I can see a future where patients do contact their pathologists every once in a while to talk about their reports.”
The volume of email is large and the team responding is small. “We do our best to get back to people,” Dr. Wasserman says. “One thing that’s been nice to see is that we get a lot of email from pathologists, researchers, other doctors from all over the world who ask to use our articles and images in their lectures and other patient material.”
The site’s content steers clear of treatment and management, as do the pathologists when they communicate with patients. “There will be for some time pathologists who worry that we are going outside our area of expertise, and we need to be cautious about this.” But he challenges those who believe “it’s best left to clinicians to try to explain the pathology report.”
“They’ve been explaining our pathology reports to patients for years, but it’s our report, in the sense that we know it best,” he says. The website is not about going into the sphere of clinical colleagues. “It’s more about helping them in their sphere. By providing this information, we’re supporting their interactions with patients.”
In building the site, he wasn’t trying to step on toes, he notes. “I wanted to explain our side of medicine to patients. And I felt that just like every doctor has a role in explaining their specialty to patients, pathologists have a role in explaining their work to patients.”
A[/dropcap] common question Dr. Wasserman and his team receive is, “Where is my diagnosis?”
“Patients copy and paste their entire report, send it to us, and say, ‘What does this mean? Where is my diagnosis?’ They don’t even know where to start,” he says. Other patients zero in on a different component of the report, thinking it’s the diagnosis when it isn’t. “It’s something in the microscopic description, or it’s the clinical history they’re seeing or something else.” Patients sometimes look for words they think are important; if the clinical history mentions melanoma, for example, and a patient recognizes the term and knows their doctor was concerned about it, they may mistakenly assume the diagnosis is melanoma even if it’s basal cell carcinoma or something else. “Especially if it’s higher up in the report,” he notes.
Dr. Wasserman thinks pathologists should make a practice of putting the final diagnosis at the beginning of the report and making it as prominent as possible. In his own reports, he puts the diagnosis in bold and in all capital letters. “And I try to put all the extra information later on in the microscopic description or comments section.” Another good practice: Within the diagnosis section, list the most important specimen first. “We have diagnosis sections that often list multiple specimens. The most important specimen might be specimen five, and then specimens one through four list extraneous stuff that doesn’t matter to the patient’s care.”
Pathologists have leeway to make their reports easier for patients to understand, he says. “You need to list the specimens you received. You need to talk about each. But that doesn’t mean you have to list them up front and bury the diagnosis.”
There’s added security for the health care system and physicians, too, when patients understand their laboratory results. If a busy physician overlooks the line in a patient’s report about a positive margin, for example, and the patient is aware of it and knows it means some of the tumor may have been left behind, “it catches an oversight before it happens,” he says. “It’s yet another layer in the Swiss cheese model of medicine, and the patient is an important part of that model.”
Though patient-friendlier reports would be helpful, patient education is the easier path, in Dr. Wasserman’s view. “Trying to get everyone on the same page to write things in a more patient-friendly way and to do things in a standardized text or format is going to be tough to achieve. I think patient education and resources are probably the first thing to go for,” he says. He puts the link to the website in his reports and says others can
do the same.
Just how tough it can be is clear to Mark Kilgore, MD, associate professor, Department of Laboratory Medicine and Pathology, UW Medicine, Seattle. He’s part of a multidisciplinary team at the University of Washington School of Medicine that is studying the benefits of and barriers to creating patient-centered versions of pathology reports.
The study’s primary investigator, John Gore, MD, MS, a urologist, became interested in pathology reports from a surgeon’s standpoint, Dr. Kilgore says. “He was finding it challenging at times to convey the pathology report to the patient,” and wanted to know: “How could we create pathology reports that are more understandable, both to surgeons and to patients?”
The team developed and piloted the patient-centered pathology reports (PCPR) for four cancer organ sites: prostate, bladder, breast, and colorectal polyp. Gynecologic tumors are next on the docket, says Dr. Kilgore, who became involved with the study as the breast pathology lead at UW. The long-term goal is for the reports to be implemented in clinical care—likely within the next three to five years, he says. As with most things in health care, he adds, it comes down to “time and money.”
In each pilot, patients were randomized to receive the standard report with or without the patient-centered version. They were surveyed at the time of pathology disclosure and one month later to assess PCPR efficacy, knowledge about their cancer, and provider communication and empathy (Austin EJ, et al. Cancer Causes Control. 2023;34[4]:399–406).
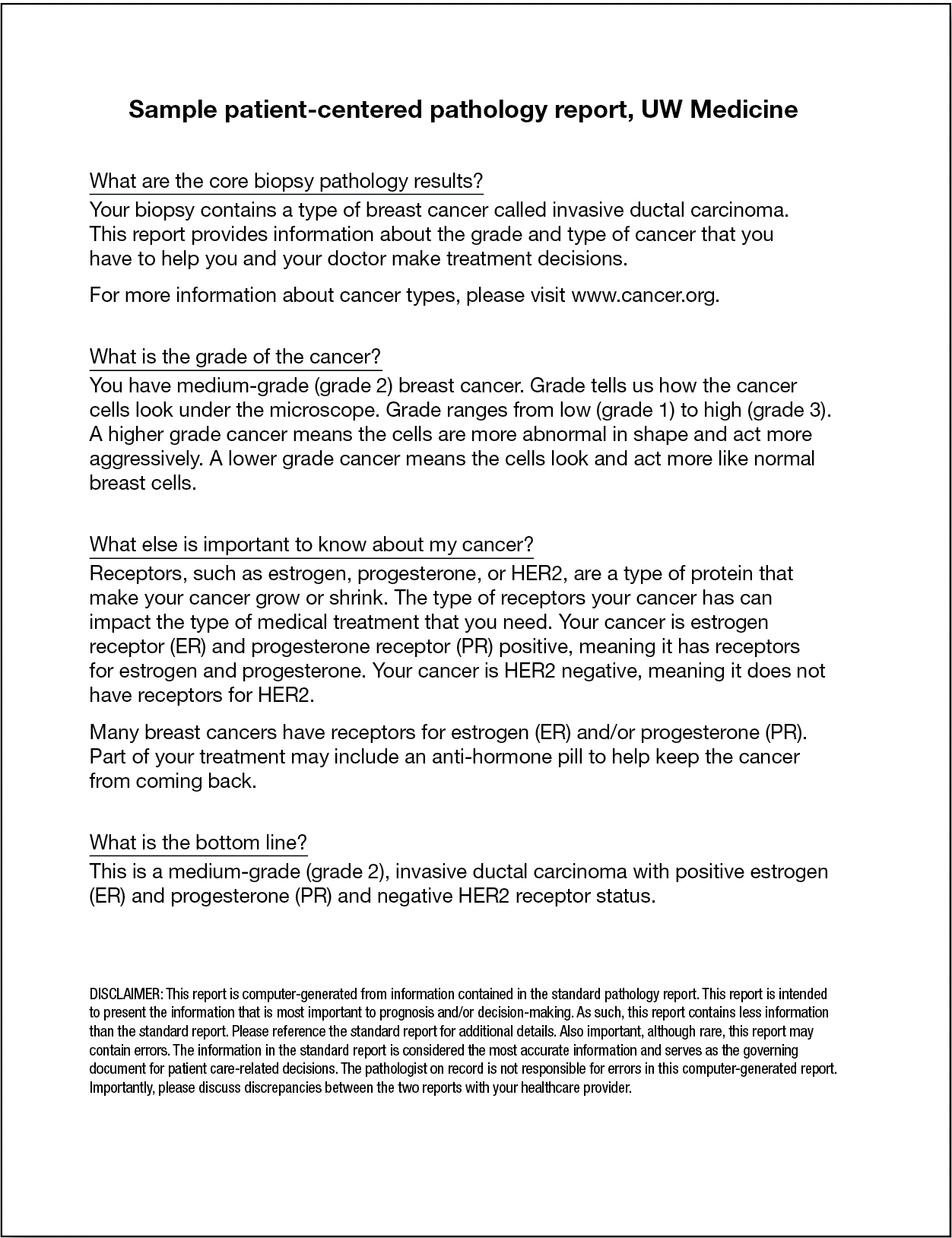
The patient-centered reports are generated from the information in the standard pathology report, but they’re brief—a breast core needle biopsy report, for example, is only a half-page long—and they include only the elements most relevant to the patient, such as diagnosis, grade, and hormone receptor status (sample PCPR, below). The reports are written at the sixth-grade reading level and follow a question-and-answer format. Grade, for example, is described as “how the cancer cells look under the microscope.”
The reports also include links to vetted resources, Dr. Kilgore says, such as those provided by the NCCN, CAP, and ASCO. “So the patients could go right to those resources, rather than search ‘metastatic breast cancer’ in Google and get a whole range of information.” Developing a separate report was more practical than modifying the standard report, he says, noting it would be difficult to satisfy national reporting requirements in language written at the sixth-grade level.
Across pilots, the patient-centered reports were shown to improve patient satisfaction, knowledge, and quality of shared decision-making. Seventy percent of patients in the PCPR arm of the colorectal polyp pilot reported that the PCPR helped them better understand their results, for example. And in the breast cancer pilot, 79 percent of patients who received the PCPR believed it helped them better communicate with their physician.
The team hired a full-time IT employee (made possible by the grant the urologist obtained) to develop an automated system to generate the patient-centered reports, Dr. Kilgore says. PCPR templates that followed the existing clinical templates for pathology reporting were built into the laboratory information system. “When we selected certain options in our synoptic ASCO/CAP templates, it would automatically generate the patient-centered language to match it,” Dr. Kilgore explains. After signing out the standard pathology report, pathologists would go into an addendum and generate an accompanying PCPR with a single click. “We envisioned a system moving forward where if you wanted to, you could release both reports on a patient simultaneously without the pathologist having to do any more work.”
The system was able to generate a PCPR in more than 90 percent of cases. Of 66 patients enrolled in the breast cancer pilot, reports for three patients with surgical pathology could not be generated due to clinical complexity or because some clinical features, such as hormone receptor status, were reported in nonstandard ways that could not be integrated into PCPR algorithms. They removed those cases from the study population.
To accommodate the more complex cases, “you would have to employ artificial intelligence—some sort of AI platform that learns as time goes on,” he says. “If you check boxes in the templates, and you can automate the language that comes out of that, that’s relatively easy to do with basic computer programming.” A rare or atypical tumor for which language has never been developed in the system would present a problem, he says. Positive or negative margins would be straightforward, “but you run into problems when the answer is ‘margin status: see comment,’ and the comment says, ‘There’s an atypical group of cells near this margin, indeterminate for cancer, may represent a positive margin,’” and a discussion comes out of that. “That’s almost impossible to automate. That’s where AI would have to come in and at least flag you if it wasn’t able to decipher the report.”
Developing the language for the breast cancer pathology PCPR templates was a yearlong process, Dr. Kilgore says, with oncologists, surgeons, and pathologists meeting monthly to discuss and critique the patient-centered language. “Pathologists are particular about their language, and even within pathologists, they’re particular about language. So we went through many rounds with the surgeons,” he says. “And all of that was filtered through patient advocates who felt strongly about some items that we would never have even thought of.”
One example: Patient advocates suggested using size comparisons, for those who might have difficulty visualizing tumor size. “Patients had advice like, ‘You could say it’s about the size of a grape.’ So we would measure grapes and say, ‘A grape on average is about 2.5 centimeters.’ And so, a tumor, if we put in that it was about two centimeters, it would automatically populate, ‘Your tumor is about the size of a grape.’”
Some of the department’s breast pathologists declined to participate in the study. “They didn’t want their reports changed after the fact or even real time into different language they felt they would have to be responsible for—now you have two reports out there, and you’re responsible for both of them.” The team included a disclaimer on the patient-centered reports that says the standard report serves as the governing document and the pathologist on record is not responsible for errors in the computer-generated report. Each PCPR was checked for discrepancies, but Dr. Kilgore is aware that creating two reports “goes against one of the fundamentals of pathology, which is only report information once. As soon as you start reporting it twice, it’s like a person with two watches—they don’t know what time it is because they have conflicting answers.”
There’s little potential for automated PCPRs to be implemented widely in clinical practice without nationwide standardization of pathology reports. “I can’t see any other way you could create a system able to interpret that many different ways of reporting things,” Dr. Kilgore says. Standardization of language and terminology would be a good start, he says. “People should be using WHO terminology, or NCCN, CAP/ASCO terminology—things that can be standardized across the country.”
Most institutions, too, lack the funds needed to develop an automated system. A company like Epic could develop such a system and make it available as part of the LIS, he says, but finding consensus on the patient-centered language among all stakeholders still would be difficult. “There’s five of us breast pathologists, and in the end, we couldn’t get consensus from all five people.” Though the final group that participated in the breast cancer pilot did reach agreement, “doing it across a larger scale—it’s hard to imagine.”
Another option, and perhaps a more realistic one, would be to develop a standalone, LIS-agnostic program, similar to Google translate, in which patients could scan their reports with a smartphone to automatically and in real time “translate” the report into patient-centered language. “It wouldn’t matter where you are or what system you’re using,” he says. “That would probably have a higher likelihood of success.”
Charna Albert is CAP TODAY associate contributing editor. Dr. Wasserman welcomes hospitals to provide a link to the website from their patient portal; he can be reached at jwasserman@toh.ca.