
Anne Paxton
September 2023—Ambiguities, inconsistencies, omissions, and other defects in the naming of laboratory tests can send test orders and results interpretation awry, particularly with some of the most common tests. Even among clinicians and laboratorians working at the same hospital for years, smooth sailing is not guaranteed.
The authors of a study published in Archives of Pathology & Laboratory Medicine hope to change that (Carter AB, et al. Arch Pathol Lab Med. Published online May 3, 2023. doi:10.5858/arpa.2021-0314-OA). Their aim is to alert patient-facing providers and laboratories to the risks that ambiguous or nonstandardized laboratory test naming poses and to provide practical rules for minimizing those risks.
“A better naming system is imperative,” write coauthors Alexis Carter, MD, Andrea Berger, MAS, and Richard Schreiber, MD.
In practicing over the years, “Dr. Schreiber and I had noticed some pretty egregious naming practices for certain laboratory tests,” says Dr. Carter, a physician informaticist in the Department of Pathology and Laboratory Medicine, Children’s Healthcare of Atlanta. (Dr. Schreiber is an informaticist and internist.) “Even with names that are ubiquitous, it’s kind of a persistent problem everywhere.” For example, “A CBC is a CBC, except that some places will include a differential and others will not.”
Dr. Carter has seen hepatitis C viral load as a test name, “but what it didn’t include was that it was going to reflex to an HCV genotype if the result was greater than 1,000 copies per mL. Because the reflex test was not in the name of the test, providers were also ordering HCV genotype,” leading to duplicate charges that had to be corrected.
The more complicated and unusual a test is, the more likely it will be subject to naming problems, although those problems are not always easily solved by changing the test name, Dr. Carter says. At Children’s Healthcare of Atlanta, “when we have a child suspected of mumps, there are three different tests you have to order on that patient and send to the state. There’s no way, in the name of the test, we would ever be able to communicate that this is part one of three tests to order. We use order sets where we can write in more information about suspected mumps. Otherwise the providers wouldn’t know they need two blood samples and a urine sample for this patient.”
Children’s has comprehensive order- and result-naming procedures, each 10 to 12 pages long, and a third naming procedure for allowed and prohibited abbreviations and symbols. Synonyms and keywords aid searches for orders. “But for what we call the formal name of the test order, we want that to be kind of the pristine representation of what that test does,” Dr. Carter says.
They also want it to be concise. “We like to keep our test names clear, but we like to keep them as short as possible. Epic, the EHR we use, allows 255 characters for a test name. But that’s going to be too long for someone to read. It also causes problems when you have a spreadsheet view of results.”
Though long touted as a solution, the federally required Logical Observation Identifiers Names and Codes fail to address lab test naming weaknesses. “There are 978 LOINC codes that come up for glucose, so you can see why someone might have trouble picking the right LOINC code,” Dr. Carter says.
Laboratories are required to assign a LOINC code to every test in their dictionary, but “there is no requirement for us to actually use the LOINC code for anything. That’s good because LOINC has serious flaws that can make it unsafe for use in patient care,” she says. For example, tests with different reference ranges can have the same LOINC code. “So a provider could think a patient’s value is going up or down when in fact it could be doing the opposite.”
Prior studies have shown that certain categories of tests can be particularly problematic, among them proteins, coagulation, blood banking, and genetics, she and her coauthors write.
There is continuing debate about who should steer the naming of laboratory tests, with some believing that patient-facing providers should name the tests. They should have input on what might confuse them, Dr. Carter says, but there can be nuances to laboratory testing, and if naming is left entirely to clinicians, “we may not have sufficient detail in the test name.”
A laboratory-provider partnership is needed, she says, but more essential would be for each hospital to have a formatting style guide, which many do not have. Dr. Carter has worked in institutions where one-third of tests to be done on urine have “urine“ as the first word, a third have “urine” in the middle, and a third have “urine” at the end.
Addressing this inconsistency is an informatics issue, she says, “because it has to do with the concept of usability, meaning that with no training somebody can go in and intuitively, automatically understand where things are going to be.”
In the study, health care providers across various specialties and perspectives completed a 38-question survey that asked for demographic information and their preferences for test names and the display of results.
The survey provided real-life examples of poorly named lab tests that the participants were asked to decipher. Participants were also asked about vitamin D test names to determine whether they performed comparatively with other published data on vitamin D test naming—“that is, poorly,” the authors write.

They distributed the survey to the Epic Smartserv user group and to professional societies, including the Association of Medical Directors of Information Systems, Association for Pathology Informatics, Association for Molecular Pathology, and Society for Pediatric Pathology, and to working groups within the American Medical Informatics Association that included physicians, nurses, and others. It’s not possible to determine the number of people who received the call for participation because of the mechanism in which the survey invitation was distributed, the authors write, noting it’s a limitation of the study. Of the 269 respondents, 162 completed the survey. Of those 162, 83 were physicians without lab or pathology experience, 40 were pathologists and physicians with lab expertise, 19 were nonphysicians without lab expertise, and 20 were nonphysicians with lab expertise.
Survey participants were grouped and compared by profession, level of training, and the presence or absence of specialization in informatics, laboratory medicine, or both.
Coauthor Andrea Berger, biostatistician in the Department of Population Health Sciences, Geisinger Medical Center, Danville, Pa., was primarily responsible for the study’s statistical analysis of respondents’ answers—in particular the differences among physicians and nurses, laboratory personnel, and people with an informatics background. “We first developed statistically significant thresholds or P-values for each group comparison, then determined how responses differed by profession,” she says. For example, laboratory-trained and informatics-trained survey respondents were far less likely than those without such training to answer “I don’t know,” when asked to decipher complex test names. On the other hand, respondents overall were consistent in rejecting abbreviations and obscure test names.
With the names of vitamin D tests, the survey found that laboratory experts fared “no better and sometimes worse” than nonlaboratory physicians and nurses, “indicating that these tests are confusing for everyone,” the authors write. One question asked participants to mark all the tests that are the same, maybe the same, or different from vitamin D (25-[OH]) serum. Listed for comparison were vitamin D (25-[OH]) serum, total; vitamin D2 (25-[OH]), serum; vitamin D3 (25-[OH]), serum; and hydroxycholecalciferol. Physicians of all specialties and nurses were more likely to differentiate vitamin D3 (25-[OH]) serum from vitamin D (25-[OH]) serum, whereas nurses and PhD nonphysicians, especially PhD laboratorians, were more likely to differentiate hydroxycholecalciferol from this term, the authors report.
Among the survey’s many other findings is the following sampling of participant preferences:
- Mixed upper- and lowercase letters for test names are favored over all uppercase letters.
- Logical categorization, not alphabetical, is the preferred sort order from top to bottom.
- Structured string architecture for names is preferred: analyte first, followed by attributes such as specimen type, antibody, and fasting (for example, prolactin level fasting or troponin T high sensitivity).
- In drug levels, the word “level” after the drug name is preferred, presumably to distinguish a drug level from a medication order, the authors write.
- For antibody tests, they prefer use of a simple IgG or IgM after the antigen name without prefixing with “anti-” (exception: anticardiolipin IgG). (Because some tests detect antibodies of antibodies, the authors advise against the use of “anti” in front of the antigen name.)
- For reflex testing, they prefer to have the name of the reflex tests with the initial test (for example, TSH with reflex T4).
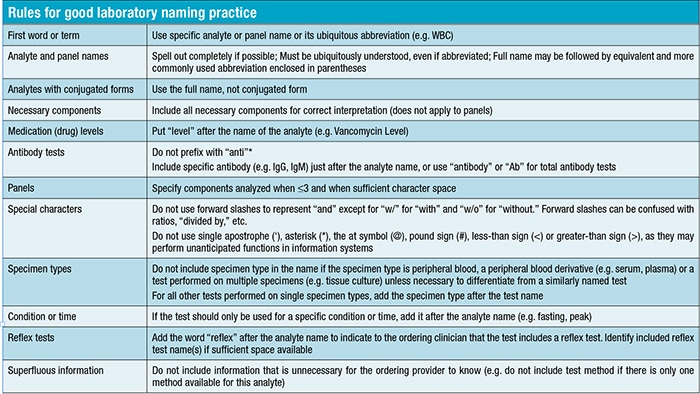
Dr. Carter and Dr. Schreiber’s rules for good lab test naming practice (see table below) were developed before the study was conducted and are used at their institutions. They used the survey to evaluate the utility of the rules as a communication tool. Participant answers align with many of the rules.
Dr. Schreiber, now a retired associate chief medical informatics officer at Penn State Health, formerly at Geisinger, is an associate in the Department of Biomedical Informatics and Data Science at Johns Hopkins University School of Medicine and professor of medicine at Geisinger Commonwealth School of Medicine.
He discovered the risks of laboratory test naming several years ago when he was working with others to institute an electronic health record at the hospital where he was chief medical informatics officer. It should be easy, he thought, to start the project using laboratory tests. “Because here’s the name, here’s the result. Now you can move it from here to there. But I was naïve.”
What were the biggest problems? “It was a combination of things,” Dr. Schreiber says. “First, it was the display of results. For a question as simple as whether to put the date on the side and the laboratory test name on the top horizontally, or reverse the two, I had certain ideas and people disagreed with me.”
A basic issue was how to get a display that has the maximum amount of information without overloading the user’s eye, he notes. “So, for example, ‘Potassium’ is a lot longer than ‘K.’ All clinicians and nurses know what ‘K’ is. But more complicated tests can have more obscure names. ‘AMA,’ for example. Does everybody know what that is? Maybe not. Or nucleocytoplasmic antibody?”
Patients are particularly unlikely to understand what names like these might signify. Two decades ago, he says, it was primarily clinicians and nurses who needed to understand the test names. “It wasn’t until roughly 2012 to 2015, with meaningful use and patient portals coming on, that we had to consider the patient. But after it became clear that we should be sharing all this information with patients, now we have a tripartite consideration—and their needs, their knowledge, are all different.” Adding to the problem is that patients have virtually immediate access to their medical records without any explanation in some cases. “And I think those records need to be more patient-centric.”

The problem with laboratory test names is a long-standing one, Dr. Schreiber says. “It’s always been bad, but it’s become more evident. One of the things I learned very early about digitization of records and keeping things electronic is that it shines a bright light on problems you probably didn’t even think about before. Because the problems immediately become evident to many people, rather than just one person who is looking at an entry in a written record that they can’t read. Now everybody sees it.”
And local institutions have their own naming standards, as do the large reference labs. At one local lab, Dr. Schreiber took a deep dive into listing all the different lab results possible on a spreadsheet and found several that were clearly the same and coded slightly differently. “Consider if someone ordered CBC, then someone else put ‘auto. CBC,’ while someone else put ‘CBC D.’ After a while, when I put the spreadsheets together, a test might have three, four, or five different possible ways of entering it into the lab information system, so they all appeared on different lines and it was hard to compare the result. Is there a difference in method or reference ranges?”
He and Dr. Carter side with estimates that 10 percent or more of lab test orders are lost or not understood properly, and the worst part may be that so much of the error problem goes unnoticed, Dr. Schreiber says. “Some lab results are never found because the person is looking for x and it’s called y and they may forget about it or never be alerted to it. Or it hit their inbox but they didn’t recognize what it was.”
Another naming-related problem is when the provider doesn’t understand the significance of the test he or she has. “Parathyroid hormone comes to mind. Did you really mean the native PTH? Did you mean the N-terminal, or were you really looking for parathyroid hormone-related peptide, a cancer marker? Maybe you think you’ve ordered a cancer marker, and you ended up with a PTH level that’s normal.”
Clinical decision support can cause other problems, Dr. Schreiber says. “One lab result isn’t always in isolation. Let’s say you want to prescribe a diuretic. Good clinical decision support will also alert you that the potassium is 3.2. You’re going to make that worse. Did anybody look? Or, more importantly, does the clinical decision support pull that info into the med order so that you can prescribe the potassium at the same time, or something along those lines?”
Computerized provider order entry has had mixed effects on the lab test naming issues, he notes. “People often can’t find the test they think they know the name of. Many times I’ve had clinicians call me and say, ‘I can’t find’ fill-in-the-blank.” His best example comes from radiology.
“It was an ultrasound, a renal arterial Doppler study. But it wasn’t under ‘Doppler.’ Or ‘renal.’ The clinician said it wasn’t under ‘arterial,’ it wasn’t under ‘peripheral.’ Where is it? So we had to create a lot of synonyms for radiology studies to develop naming conventions, and then it was much easier to find.”
For lab tests, however, creating synonyms is not easy, Dr. Schreiber adds. “If I order potassium, for example, I’m going to get a long list which might include potassium hydroxide, for a vaginal smear, a KOH test. I can find the word, but not the test I’m looking for. So you need a system with more guidance in it. And the keywords have to be clearer.”
Vitamin D is tricky, he says, partly because of the lack of appropriate knowledge among clinicians. “But total vitamin D is adequate for almost every patient except perhaps those with severe renal disease or those where you’re considering osteomalacia or that sort of thing.”
Nevertheless, he sees test orders for vitamin D total, vitamin D2 or D3, hydroxy vitamin D, and so on. “It’s extraordinarily confusing.”
Cognitive research makes clear a key advantage of improved naming conventions, Dr. Schreiber says, and it relates to being noninterruptive of cognitive processes and not contributing to alert fatigue.
When a clinician is ordering a test, “you’re thinking about a problem, you’re interpreting what the patient needs, and you’re making a decision about an order. If you’re interrupted at one of those points, you’re disrupting the thought process and therefore prone to error.”
In his experience, the most disruptive setting in which this occurs is in clinical decision support, where the clinician may complete a test order menu for all the x-rays, lab tests, and medications. “Then I need to add a CBC because I’m going to need it tomorrow and get the message ‘You’ve got a drug/drug interaction.’ So in going back to redo the orders, you can take out an order inadvertently or you can add an order that’s now another alert-provoking action. So it’s a cognitive problem that’s a safety issue.”
There is consensus among provider organizations that a single, clear naming strategy for laboratory tests is achievable, the authors write. Asked whether he agrees with the consensus, Dr. Schreiber says he and Dr. Carter are optimistic. “Laboratory personnel are health care workers who have the best interests of patients in mind, and we all want to do the right thing. And we want to make things comprehensible for each other and our patients and their families.”
As research continues, he would like to see not only better publicity about the work that is currently being done on naming conventions but also prospective research studies. “They could compare the efficiencies of naming something x versus y and see what clinicians like better in real life. Have half of the staff see one name, half see the other, and then survey and see which one works better.”
“You need to ask bedside clinicians who use lab test names every day, who are at both ends of the spectrum,” in that they’re ordering a test and looking at the result, Dr. Schreiber says. But he adds a caveat: “Nonlaboratory doctors and nurses are not the experts here. The lab is.” So lab test naming “needs to be a close collaboration between what the doctors think they need and think they want to see and the lab saying why this is a good or not a good thing.”
Dr. Carter notes that TRUU-Lab, an initiative based at Texas Children’s Hospital, has in recent years brought together health care providers, professional societies, and industry groups to address problems caused by ambiguous, incomplete, and nonstandard lab test names. “My work is kind of happening independently of that,” she says. And one of her goals for future work is to take the style guide she has developed and make it computational.
“I’d like to be able to have a tool asking what is the analyte name, what are the specimen types, and other questions, and then have the tool name the test and see how well that works.” If you can develop a tool like that, she says, “it will make lab test naming a lot easier for people.”
Anne Paxton is a writer and attorney in Seattle.