
Sherrie Rice
April 2023—Molecular testing guidelines say that the neoplastic cell content of each specimen should be assessed, but there are no formal recommendations or guidelines on how to do the assessment.
Last year, current and past members of the CAP Molecular Oncology Committee set forth 13 recommendations, beginning with the definition of neoplastic cellularity and ending with quality assurance (Devereaux KA, et al. Arch Pathol Lab Med. 2022;146[9]:1062–1071). In an AACC session, Joel Moncur, MD, PhD, MS, a member of the committee and director of the Joint Pathology Center, Silver Spring, Md., explained why.
“Assessing neoplastic cellularity is an imprecise process, and we knew that because of a study done by the Molecular Oncology Committee” and reported in 2013, he said (Viray H, et al. Arch Pathol Lab Med. 2013;137[11]:1545–1549).
It was a prospective, multi-institutional diagnostic trial that found “there was low interobserver precision among pathologists and laboratories for the assessment of the percentage of neoplastic cells. In fact, in over half of the cases that were part of that study,” he said, “more than 10 percent of the participants overestimated neoplastic cellularity, which puts them at risk of a false-negative result.”
Insurers will often reimburse for mutation profiling only one time, Dr. Moncur said. “So if a test is conducted on an insufficient sample and the mutation is missed, then that patient may never again be offered the opportunity to be tested, and thus could miss the opportunity for a life-extending or lifesaving therapy.”
More recently, in 2019, the committee designed a questionnaire and performance challenge to help explain why neoplastic cellularity assessments can be imprecise. “And we discovered amazing things,” Dr. Moncur said.
They found that laboratories are using different methods to assess neoplastic cellularity, and CAP proficiency testing data makes clear that different methods produce different results. Laboratories also are using different definitions of neoplastic cellularity. Seventy percent of the 57 laboratories from which data were derived appropriately use the cell number method: the number of neoplastic cells compared to the overall number of cells in the tissue that will be tested. But 28 percent of laboratories were using the cell area method: the area of neoplastic cells compared to the overall area of the tissue. Defining neoplastic cellularity by cells or nuclei is considered to be more accurate because the number of cells or nuclei correlates directly with DNA content.
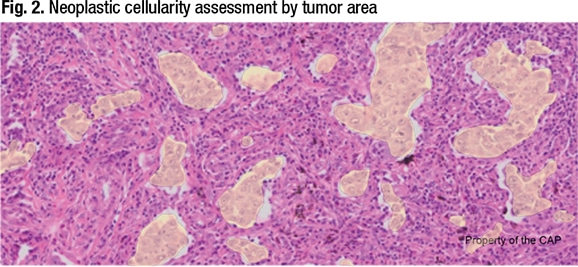
In Fig. 1 is an image of a lung cancer. If the laboratory’s molecular assay requires samples with at least 20 percent neoplastic cellularity, Dr. Moncur asked, is this specimen adequate for testing? The answer, he said, is no.
If the tumor cells in the Fig. 1 image of lung carcinoma are highlighted (Fig. 2) and the area method is used, “we could easily get to 20 percent neoplastic cellularity and call this specimen adequate. But that’s not the right way to do it,” Dr. Moncur explained, “because the DNA content of tumor is based on cell number as opposed to cell area. So this is how we determine the criterion standard, or the gold standard, for determining neoplastic cellularity, which is the number of neoplastic cells compared to the number of benign cells.”

In Fig. 3 is a demonstration of how the Molecular Oncology Committee develops the criterion, or gold, standard for each image. A red dot is placed over every neoplastic cell in the lung carcinoma image and a green dot over every benign cell in the background—292 red dots and 2,855 green dots, which is a 9.3 percent neoplastic cellularity. “So it’s important for laboratories to rely on cell number, which may be difficult when you have very large neoplastic cells and very small lymphocytes and other benign cells in the background, but that’s the best method to use to assess neoplastic cellularity,” he said.
That same image of lung carcinoma was presented to a group of laboratories, “and we found that labs that assess cellularity by tumor area were much more likely to overestimate.” So the advice is to define neoplastic cellularity as the number of neoplastic cells or nuclei compared to the overall number of cells.
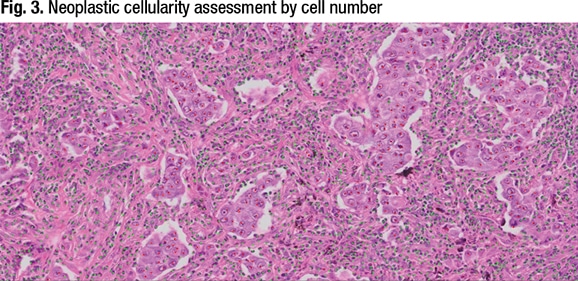

Fig. 4 is a breast mass specimen that is not adequate for testing. “This case relates to the issue of whether or not you should include in situ carcinoma in your assessment of neoplastic cellularity, and this is another area where we determined there was a difference among laboratories,” Dr. Moncur said. Seventy-four percent do not include in situ carcinoma in their assessment of neoplastic cellularity, and 17.5 percent include it. The image is predominantly ductal carcinoma in situ of the breast, and it is within a preexisting duct of the breast. “It’s lined by myoepithelial cells around the periphery, so this is a proliferation of epithelial cells within an existing duct, and thereby a diagnosis of ductal carcinoma in situ,” he said.

The only invasive carcinoma that’s present in this part of the specimen is on the right side of the image, top, and it makes up only three percent of the overall cells when all cells on the slide are counted, he said. It raises the question: What to do? Should the in situ carcinoma be included or not?
“What we did find out, through our performance challenge, was that laboratories that choose to include in situ carcinoma had a much higher estimate of neoplastic cellularity compared to labs that do not include in situ carcinoma, again making the point that different methods lead to a different result, and we need to eliminate that variability if we’re going to do this well.”
Laboratories need to be cautious if they’re going to include in situ carcinoma, he said, “because mutations may or may not be conserved between the in situ and the invasive part of a tumor.” Genes like PIK3CA, if they’re mutated, are conserved between ductal carcinoma in situ and the invasive part of the tumor. “But HER2, as an example, is a gene where there’s oftentimes a discordance where there could be amplification of the HER2 gene just in ductal carcinoma in situ and it’s not present in the adjacent invasive carcinoma. So this is a vulnerability, and again an area where we detected method differences that affect the results of the test.”
The committee uncovered other data of interest, Dr. Moncur said. Most laboratories excluded apoptosis and necrosis in their assessment, for example, but some laboratories “included or were unsure how to assess such features,” he and his coauthors wrote.
“Extracellular mucin is another feature that could potentially affect neoplastic cellularity assessment, particularly for laboratories that define neoplastic cellularity based on tumor area,” they continued. Of the 16 laboratories that determined neoplastic cellularity by area, 12 excluded extracellular mucin. Two included mucin, and two were unsure whether mucin was included in their assessment.
Among the committee’s other findings:
- More than half of the laboratories (31 of 57) refrained from testing when the neoplastic cellularity was below the determined minimum percentage cutoff or limit of detection. Twenty-two of the 57 labs proceeded with testing when the neoplastic cellularity was below this cutoff, and the threshold for testing varied by laboratory “and likely depended on the molecular assay used,” the authors wrote. Four of 57 said they had no minimum cutoff.
- More than 80 percent of the laboratories used neoplastic cellularity either consistently (26 of 57) or occasionally (21 of 57) in the postanalytic interpretation of results.
- When no variants were detected, 36 of 56 laboratories routinely or situationally re-reviewed the neoplastic cellularity.
The committee members used all the information they gathered to develop the initial set of recommendations (Fig. 5), one of which is that a qualified pathologist should review all such assessments. It is a CAP accreditation requirement (MOL.32395), Dr. Moncur noted, because pathologists “are trained to recognize the subtle morphologic features that make the diagnosis, so you know exactly what it is you’re putting into your sequencer or assay.”
Another recommendation: Any limitations of a molecular assay based on the neoplastic cellularity assessment should be noted in the molecular report. “So patients have the opportunity to perhaps have that tissue retested and identify something that could change the course of their disease,” he said.
Sherrie Rice is editor of CAP TODAY.