
Karen Titus
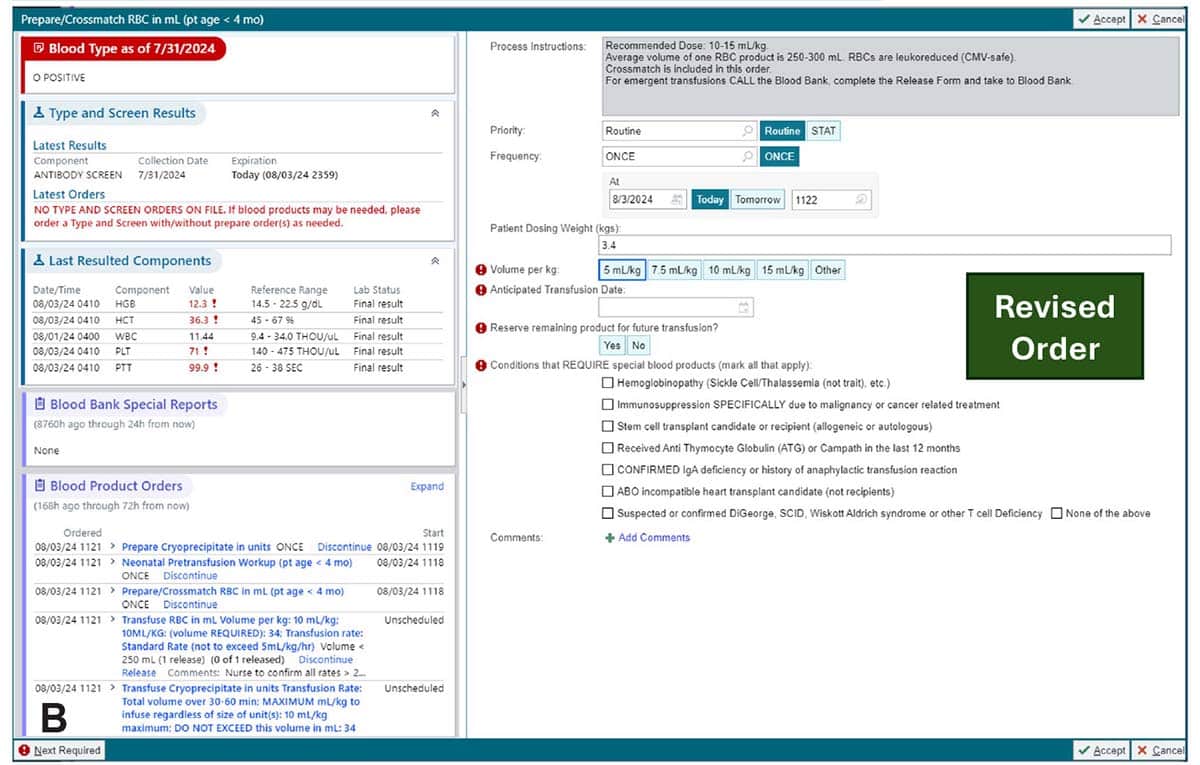
October 2025—For all the effort, redos, build-outs, planning, talking, and time that went into revamping blood product orders at Children’s Healthcare of Atlanta, the essence can be distilled into Fig. 7 of a recently published article on the project (Rollins M, et al. Arch Pathol Lab Med. Published online June 25, 2025. doi:10.5858/arpa.2024-0074-OA).
The figure shows the differences before and after optimization for a single prepare order. The minimum required clicks dropped from seven to four, and the revised order now displays the patient’s blood type, current blood product orders, and whether the antibody screen is still active. It also no longer requires advanced transfusion medicine knowledge. If there were a caption to describe how orders became more streamlined and intuitive, it could read: “Think less.”
Obviously no one wants health care providers, either in the blood bank or at the bedside, to play dumb. But, says coauthor Alexis Carter, MD, the right people need to be thinking about the right things, as opposed to second-guessing routine steps, considering clicks, and trying to remember arcane transfusion rules.
“This is the fundamental premise of this paper—that patient-facing physicians [are asked] to have expertise in transfusion medicine when placing orders,” says Dr. Carter, physician informaticist, Department of Pathology and Laboratory Medicine, Children’s Healthcare of Atlanta, and program director, Emory clinical informatics fellowship program. “Which is not realistic for most physicians.”

Asking providers to remember such intricacies when they place an order didn’t necessarily make sense.
But for others, this is everyday knowledge. “The blood bank knows. I’ve been saying that for years,” Dr. Carter says.
The essence of the yearlong overhaul at Children’s, which went live in August 2022, was to standardize blood orders to improve transfusion safety at its two quaternary care hospitals. (The health care system also includes a smaller community hospital and eight urgent care locations.) Three years later, results have shown the power of a better order.
Take Dr. Carter’s aforementioned example. Transfusion medicine physicians and blood bank staff understand what blood product attributes are needed for various disease states, and they have easy access to patient history. It makes sense for them to manage protocols for selecting product modifications and attributes.
On the other hand, the blood bank won’t know about a patient’s current clinical conditions that might require a specialized blood product. “But the clinicians know,” she says.
That awareness led to a substantial shift. “We fundamentally changed the orders,” Dr. Carter says (as Fig. 7 shows in the article). The current order screen no longer includes prompts requiring providers to select the attributes for each product they order. Rather, they’re asked about patients’ conditions, such as immunosuppression specifically due to malignancy or cancer-related treatment, for example, or confirmed IgA deficiency or history of anaphylactic transfusion reaction. Under a single prompt, “They click off the indications the patient has, and the blood bank manages the rest,” Dr. Carter says.

Before this approach went live, the blood bank made about 15 calls weekly to physicians to clarify prepare orders, the authors note. In the first 10 months after implementation, the average dropped to four per week, and such calls now seem like a barely remembered practice, like adjusting a TV antenna.
“I will say that when the clinicians found out they were no longer going to have to figure out whether they needed to order an irradiated product, they were very happy,” Dr. Carter says.
In fact, she adds, this is the sort of change that could translate well to nonpediatric institutions. Those who take care of adult patients “are no better set to answer those questions,” she says. “It’s about letting the people who have the expertise in an area do the job.”
Another notable success was a drop in order modifications made within 60 minutes; such modifications were seen as a surrogate indicator of end-user confusion. Prior to implementation, these changes occurred an average of 34.5 times per month. Right after implementation, there was an immediate 40 percent reduction.
Another success was reducing by about half the number of ECMO order sets, Dr. Carter says (Fig. 1 in the article), through use of benchmarking and changing some of the rules.
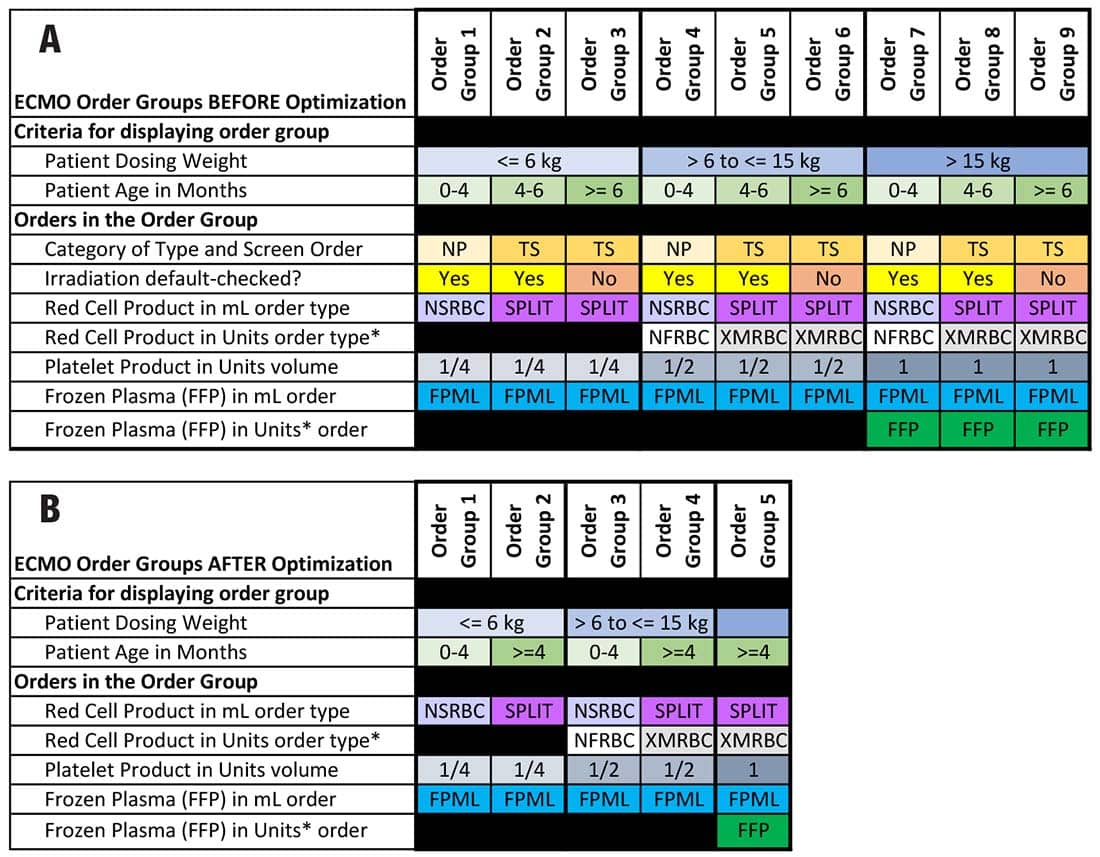
From Arch Pathol Lab Med. doi:10.5858/arpa.2024-0074-OA.
They also added clarifying language for non-OR and OR orders, after physicians told the project team that the wording was confusing. And expanding the order set better reflected additional clinical scenarios.
Perhaps most gratifying to Dr. Carter is the safety impact of the revamp. In the three years since go-live, she says, the institution has not had a single overtransfusion event.
None of this would have been possible without an overhaul, and overseeing it all was lead author Margo Rollins, MD, a transfusion medicine physician.
The project came about because of sentinel issues in the hospital, with several events occurring in a short time span, says Dr. Rollins, adjunct associate professor, Department of Pediatrics, Emory University School of Medicine, and section director for tissue, transfusion, and apheresis, Department of Pathology and Laboratory Medicine, Children’s Healthcare of Atlanta. Interest in unearthing the root causes behind the problems was high, especially since earlier efforts failed to prevent them. In fact, as the authors note, the number of transfusion-associated safety events had increased after changes were made in 2019.
It made perfect sense to target the project from multiple perspectives, Dr. Rollins says, from those putting in the orders to those receiving them. “Are we all doing this handoff correctly?”
Given her background and training as a hematologist oncologist who also works in transfusion medicine, Dr. Rollins jokes that she speaks multiple “languages”: hematology, pathology, and clinician. “Laboratorians and clinicians speak very different languages,” she says. “So we wanted to make sure that what the clinicians thought they were communicating to the laboratory was correct.” Nurses have their own language as well, she says. The institution’s large number of trainees also needed to be included.
“We had to make sure the orders were useful for everybody. We wanted to create guardrails to minimize the number of mistakes,” Dr. Rollins says.
It also needed to be user-friendly. The group did several iterations of end-user testing. Thinking something will work is one thing; making sure it does is a different matter.
The patient safety events—Dr. Rollins describes them as “not uncommon in hospitals”—were an opportunity to look at every input into the transfusion service. That included identifying “inputs we didn’t even know existed,” she says. “And then to critically evaluate that with a variety of different eyes and perspectives to get feedback on how to improve the process.”
If it sounds roughly similar to taking an entire vehicle apart (á la “Radar” O’Reilly shipping a jeep, piece by disassembled piece, from Korea back to his Iowa hometown, in one well-known M*A*S*H episode), Dr. Rollins (whose father is an airplane mechanic) suggests the metaphor is apt.
In transfusion medicine, she says, process improvements tend to fix a single process; evaluation of the fix is similarly focused. With the recent change at Children’s, she says, “The process was on steroids. We deconstructed everything to make sure that if we fixed a thing on the left, we didn’t inadvertently break something on the right.”
Earlier efforts to improve blood orders “didn’t have the desired effect,” says Dr. Carter tactfully, noting they also lacked the resources that were devoted to this most recent effort.
Both Drs. Rollins and Carter praise the leadership of Beverly Rogers, MD (who was chief of pathology at Children’s at the time and is now retired), who convinced those in the organization that the current blood ordering process needed to be improved from the ground up.
Says Dr. Carter: “She is a master at relationship building and maneuvering.” And while the project may have happened eventually without her involvement because the project was greatly needed, “I don’t know that it would have happened as well as it did.”
Dr. Rogers oversaw the various working groups, the participants of which were nurses, physicians, advanced-practice practitioners, laboratory physicians, medical technologists, physician informaticists, and transfusion safety nurses, as well as administrators representing the hospital, laboratory, and information technology. She also led efforts to garner benchmarking data from other institutions.
Taking a more comprehensive approach was helpful in unexpected ways, says Dr. Rollins. Among other benefits, it created a sense of empathy and community for those involved in the process. Nurses aren’t necessarily aware of the regulatory process involved in labeling, receiving, and testing specimens, Dr. Rollins says, and without that awareness, it can seem like “the blood bank is just dragging their feet getting your labs done.” Similarly, those in the blood bank weren’t privy to all the steps nurses are required to follow to transfuse blood.
“And,” she says, “nobody knew the complexities on the provider end.”
To revise the orders, they had to dig deep. That meant (among other things) asking providers for their pain points—as Dr. Carter puts it—when ordering blood. The responses were clear and specific—for example, having to close out an order to return to another screen to look at lab results. Vanderbilt University Medical Center—one of the institutions that provided Children’s with benchmarking data—was already using a so-called sidebar report in its orders, which eliminated the need to toggle between screens. “We basically, shamelessly, copied them,” Dr. Carter says. The sidebars are immensely popular with providers and are now included in culture orders, noting a patient’s recent culture history and antimicrobial susceptibilities.
Moreover, given the large number of trainees and varying levels of experience at Children’s, the orders needed to be built to make them clear and intuitive for users regardless of their level of expertise. Education can fill in some, but not all, gaps. “Everybody knows education is difficult,” says Dr. Rollins. “You can disseminate it from the top, but making sure it gets down into the crevices, where the mistakes often happen, can be hard.” A better goal, she says, is to make it hard for people to make a mistake.
For her part, Dr. Carter, as an informaticist, said she “wanted the build on the back to be very clean.” When there’s ambiguity in how things are named, for example, “that always leads to problems later on.”
The goal was to reduce variability and confusion, agrees coauthor Sarah Thompson, RN, MSHMI, informatics advisor and order set lead, Children’s Healthcare of Atlanta. That meant an extensive build, she says, which she oversaw. The bedrock of the design was safety. Experts build the first version. That version is then tested by those who place orders, and their feedback drives the second iteration.
Thompson too points to language issues, including different interpretations of the word “aliquot,” which, she points out, “is not part of current training for most of us.” The redesign in 2019 enabled users to order aliquots, which led to miscommunication: Did 150 mL in two aliquots mean the provider wanted two 75-mL transfusions, or two 150-mL transfusions, for 300 mL total? The latest redesign dropped the aliquot option, but providers now have the option to reserve the remainder of the unit for cases in which they want to allocate a specific unit for transfusing over a patient’s admission to limit exposure to additional donors. Providers who want to administer small, sequential transfusions now place separate orders for each transfusion—a process that takes more steps but is clearer and safer, Thompson says.

This bait-and-switch approach turned out to be effective, Thompson says. (Dr. Carter calls Thompson “the master of the bait and switch,” in fact.) “We can’t stop people from going into Epic to try to place an emergency order.” But once they start down that path, “then I can show them there is no order to place.” Thompson and her colleagues used a similar tactic when designing orders for larger patients. Some providers were still ordering in mLs, even for patients heavier than 20 kg. It made more sense to order units for such patients. “But when users were clicking around during usability testing, they didn’t want to order in units,” Thompson recalls. So she and her team directed them to an image that basically said ordering in mLs wasn’t allowed, but that they could set up a maximum volume in the transfusion order. “That gently redirects people, so they’re not thinking we forgot something.”
She and her colleagues benefited from having a human factors engineer on their team. No matter how sound the science, orders can fall apart easily when they don’t account for basic human behavior. Or, as Thompson puts it, “At the end of the day, people click where they click.”
Trying to change that simple reality will get you about as far as a trip on a hamster wheel. “But what we can do is make the relevant information more visible in the places they are already going,” Thompson says. “Because if you try to get them to do things that are outside their normal workflow or scope of practice, your success is greatly reduced most of the time.”
Another maxim: “What you see is just as important as what you don’t see,” Thompson says. That’s especially true of the sidebars.
Guardrails also help keep people on track. As Thompson notes, Children’s blood banking is set up so that users can’t order outside of the order set. “We have it locked down technically, so that people have to have a conversation” with the governance council if they want to make a change.
If it’s reasonable to characterize the rebuild as a return to clarity, it’s also fair to ask how the system became so convoluted.
Dr. Carter traces it to the basic act of someone needing a small change—well intentioned and innocuous on the surface but with no thought to its impact in, say, five years.
She offers one example out of the hundreds she says exist: a provider who misses placing an order for vitamin D testing on a patient with cystic fibrosis, then requests an alert for all CF patients for whom a vitamin D order hasn’t been placed.
That one alert seems reasonable, Dr. Carter concedes. But an alert “is kind of a quick and dirty fix,” she says. “And that’s how a lot of the complexities get written into the system.” Every new alert comes on top of countless other alerts in the system flagging minor drug alerts, allergies, and other lab orders—to the point where interruptive alerts become common and easily ignored.
The better solution, Dr. Carter says, is to find a long-term, sustainable fix that fits into providers’ workflows.
Dr. Carter walks through such a scenario. In the case of requesting the vitamin D alert, “You sit with the provider and ask a series of ‘Why’ questions,” she says:
- Why do you think the order was missed?
- Do you think the order didn’t show, or did you not remember to place it?
- Did you go into another order set to place orders on this patient? Or are you placing all of your orders one by one, instead of using an order set?
- If you’re using an order set, and you always need to order vitamin D, was that vitamin D order default checked on the order set?
It takes time to ask such questions, she acknowledges. And it takes additional time to figure out the provider’s workflow: When exactly do they need to order a vitamin D? Is it every visit? Is it every other visit? How, exactly, do they manage this?
It also takes time that IT professionals may not feel they have. “When you have an IT analyst who’s got a hundred tickets in their queue, it can be difficult to take that approach,” Dr. Carter says. Then again, redoing a task takes time as well. The lower redo rates were worth the extra time the rebuild took. “If you don’t find time to do it right the first time, you better find time to do it over.”
What surprised Dr. Rollins as she and her colleagues went through the process?
Though everyone is familiar with standard operating procedures, “they were not being followed the way we thought they were,” she says. Even with experienced staff—or perhaps in part because of their experience—it soon became apparent there was an unsettling amount of variety in following process. Familiarity with processes and patients led to caregivers skipping steps. “From the blood bank perspective, that was eye-opening. That was a shocker for me.” A recurring theme, as it turned out, was that each group worked within—and understood the process—from its own silo. And within each silo, there was variation as well.
None of this was done with ill intent, of course. Caregivers were relying on a type of muscle memory, Dr. Rollins says. When those problems became evident, it was important to reassure them that the point of the rebuild was not punitive; rather, it was to ensure they could do their own work seamlessly, safely, and accurately. She uses the analogy of car accidents, which commonly happen close to home. “That’s when you’re familiar with your surroundings,” she says, “when your guard is down, when you’re not paying attention. So we want to reinforce to people that this may be a process you’re familiar with, but your job is to be hypervigilant.”
As the Archives article notes, the process uncovered multiple, often conflicting workflows within a single department. Indeed, some nonstandard practices were embedded in the workflows of those the article diplomatically refers to as “seasoned practitioners.”
That made streamlining processes more difficult but not impossible. Dr. Rollins notes that some providers defended their personal preferences based on experience. Subsequent discussions then focused on whether there were data to support those preferences, especially given the overall goal of standardization. Even as some departments continued to insist they had special needs and thus required special orders, Dr. Rollins and colleagues would circle back to the literature or, rather, the lack of it.
But—and this was also crucial—“We didn’t make the decision for them,” says Dr. Rollins. “They were actively involved in doing the research and creating the SBARs [Situation, Background, Assessment, Recommendation framework].” Once they identified the lack of data to support what might have been, say, a 20-year practice, the next step was to question the need for the practice. Quite often, the answer was: no.
If providers doubled down on insisting a practice was necessary, Dr. Rollins and colleagues tried other approaches.
One involved looking beyond Children’s. This is where the benchmarking was invaluable. Says Dr. Rollins: “Hospitals, as much as they are all about themselves, they’re also about how they compare with their peers.” In some cases, peer data helped them identify how making a change could work: This institution you consider a peer is doing it, so what is your reservation? Pediatric institutions tend to be generous in cooperating with one another, Dr. Rollins says—that’s one reason the benchmarking data was so readily shared. She says Children’s was candid about the enormous scope of its project and asked for equal candor in return: Tell us what works and what doesn’t.
Sometimes the best approach was to meet in the middle, with an agreement to revisit the questionable practice in six months. There were very few such cases, which made waiting acceptable to Dr. Rollins and her team.
This was also well received by the insistent providers, Dr. Rollins says. “The stakeholders who were involved in those conversations felt like they were heard. They felt like they were in a position to advocate for themselves and advocate for their patients.”
Most of the troublesome practices have now been dropped. “It didn’t happen immediately, but eventually it did happen,” says Dr. Rollins. “I think the eventual part came because there was trust.
“Ultimately, that is what the entire project leaned on: trust,” she continues. “We need to trust that everybody who is supposed to do their part is doing their part. And we need to make it as easy as possible for everyone to do their part. Even if I don’t speak your language, if I trust that you will do the job correctly, then I don’t have to worry about what language you speak.” That same approach can work well outside the pediatric setting, she says. “Engaging people, and showing them the logic for the builds, will translate well to the adult side.”
Perhaps the most valuable language of all turned out to be rooted in pragmatism, Dr. Rollins says: learning to leverage the unofficial leaders at Children’s. She acknowledges this has nothing to do with blood orders or the IT system, or any of the obvious elements of transforming transfusion practices.
Initially she thought the project’s success would hinge on getting buy-in from department chairs and other obvious leaders. But as Dr. Rogers, former chief of pathology, advised her: “It’s not the chief who sways people’s opinions. It’s not the director.” In fact, because of their status, they may be further removed from everyday practices. Rather, the real leader is often a clinician who garners near universal respect. “And when they say, Nope, I’m not going to do that, everyone trusts that person” and follows their lead, Dr. Rollins says.
How did she identify those leaders? “We have the luxury of having a physicians’ lounge here,” she says. “And the physicians’ lounge, I often say, is like the high school cafeteria.” She started taking note of the informal conversations taking place there and who drew others to them. “It wasn’t the chiefs who were coming into the lounge,” she says with a laugh. “It’s also useful to reach out to your own contacts in a particular department and ask, ‘Who’s your source of trusted information? Who’s your oracle? Who’s your true north?’”
“When you continue to build relationships like that, people then become comfortable saying, ‘If you ever have questions, don’t go to this person; go to that person.’ Or, ‘This person will get the thing done,’” Dr. Rollins says. “So a good bit of what I ended up doing was relationship building. That’s what ultimately allowed this project to take off.”
Interestingly, resources didn’t come in the form of extra pay or staff. “It was a labor of love,” says Dr. Rollins. No one who participated received additional pay or time off service—or time off anything else—and no FTEs were allocated to the process. “The unofficial leaders engaged because they wanted to make the process better for their particular department. It was fantastic.”
Karen Titus is CAP TODAY contributing editor and co-managing editor.