
Charles Fiegl
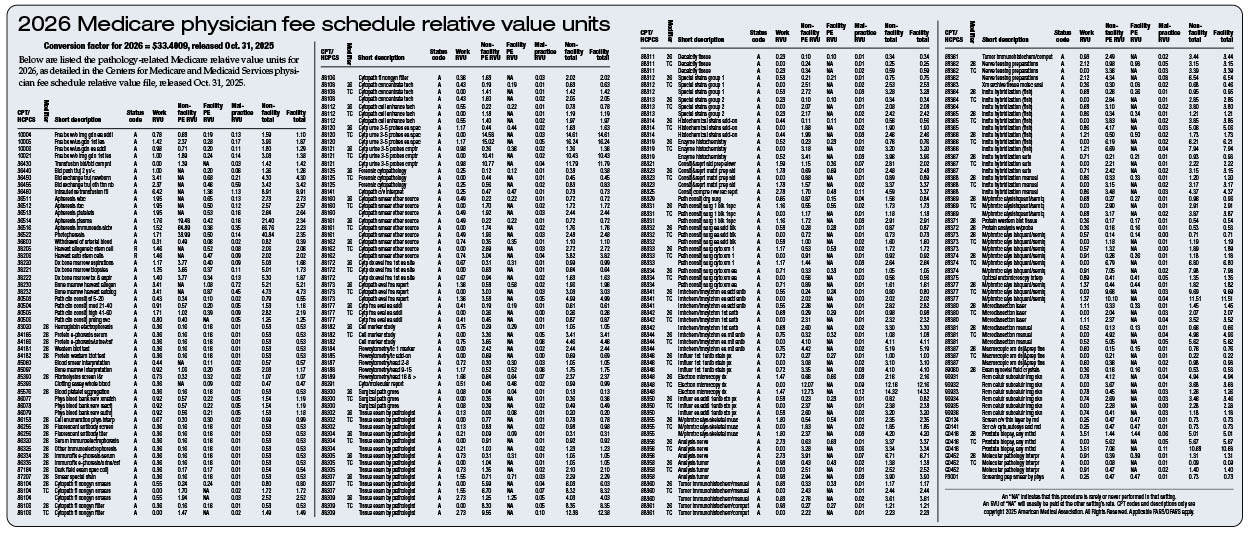
December 2025—Pathologists are set to receive a 0.34 percent payment rate increase in the 2026 Medicare physician fee schedule. However, this modest boost would have been higher if not for the application of a new “efficiency adjustment” that reduces payment rates for pathologists and other specialists by cutting physician work values 2.5 percent. The 2026 impact for individual pathologists may vary depending on their case mix (see 2026 relative value units for changes below).
The CAP, along with several other physician organizations, is strongly opposing the efficiency adjustment, which applies to more than 7,000 services representing 95 percent of all services provided by physicians. The CAP remains committed to advocating for fair reimbursement that accurately reflects the value of pathology and laboratory medicine. The CAP since July has directly lobbied both the Centers for Medicare and Medicaid Services and Congress to withdraw the adjustment.
The One Big Beautiful Bill Act, enacted July 4, provided a one-year 2.5 percent payment increase after months of congressional debate. The CAP, American Medical Association, and other physician groups had pushed for broader reforms to the Medicare physician fee schedule, including annual payment updates tied to inflation. Such reforms would eliminate the need for temporary congressional interventions to prevent cuts caused by flaws in the current payment system.
More than a week after the law was signed, the CMS released its proposed 2026 Medicare physician fee schedule, introducing the efficiency adjustment. The CMS justified the policy by claiming the current payment system does not account for efficiencies gained over time in physician work RVUs for non-time-based services. According to the CMS, as certain procedures such as surgical, radiologic, or diagnostic services become more common, physician efficiency naturally improves owing to increased experience, technological advances, and operational refinements. The CMS also said that additional efficiency adjustments may occur every three years.
The CAP strongly opposed the proposal, calling it flawed and unnecessary.
In a Sept. 11 comment letter, the CAP reminded the CMS that the statutory definition of the “work component” of physician services refers to “the portion of the resources used in furnishing the service that reflects physician time and intensity.” Applying a blanket efficiency adjustment to all non-time-based RVUs violates this statutory principle, the CAP argued. The law requires valuations to reflect the actual time and intensity of each service, not an assumed global efficiency. The CAP emphasized that a broad-brush adjustment fails to recognize the wide variability in physician services. For example, potential efficiencies gained in long, complex surgical procedures differ greatly from those in diagnostic testing or pathology. The CMS’ approach inappropriately generalizes efficiency gains that may not exist across all services, the CAP said.
The CAP further argued that the efficiency adjustment ignores the realities of modern medical practice. Physician workloads are often increasing, not decreasing, due to rising patient complexity and technological advances. Emerging tools, such as artificial intelligence, may also generate vast amounts of additional data requiring more interpretation, correlation, and validation by physicians. Likewise, complex patient cases often demand greater review and documentation time. These factors add to physicians’ cognitive and interpretive workload, rather than reduce it or create efficiencies.
In its final 2026 Medicare physician fee schedule, released Oct. 31, the CMS agreed that it had incorrectly classified certain time-based pathology consultation codes (CPT codes 80503, 80504, 80505, and 80506). These codes were subsequently exempted from the efficiency adjustment. However, all other pathology services will still see their physician work RVUs reduced by 2.5 percent.
The CMS acknowledged that technological changes affect services differently and pledged to review related data for future fee schedules. It also said the efficiency adjustment will not apply to new services for 2026.
Despite this, the CMS confirmed it will continue to broadly apply the efficiency adjustment. In response to concerns about its cumulative impact, the CMS says: “We acknowledge the concern that efficiencies may not accrue indefinitely and that overly repeated application of the efficiency adjustment could have cumulative effects over time. As such, we will continue to monitor the impact of the efficiency adjustment.”
The CAP is now urging Congress to intervene and stop the implementation of the efficiency adjustment. CAP members are being asked to contact their representatives and senators in Congress by using the CAP Action Center for grassroots advocacy at www.cap.org and discuss with lawmakers how the cut will affect them. After the final fee schedule was released, the CAP also sent a letter to congressional leaders warning that devaluing physician work RVUs could have far-reaching consequences. It said pathology physician work RVUs represent the mental effort, time, and intensity required of a pathologist in their diagnostic work to diagnose cancer and other diseases for Medicare beneficiaries. The letter continued: “This flawed policy represents a cut of tens of millions of dollars to pathology professional diagnostic services. This amount underestimates the full impact on pathology diagnostic services, as it does not include the additional loss in practice expense reimbursement resulting from the reduction in the work RVUs.”
Elsewhere in the 2026 fee schedule, the CMS announced it will not use data from the recent AMA physician practice information survey in calculating payment rates.
The CAP had urged the CMS to reject the survey’s practice expense per hour data due to small specialty sample sizes that introduced substantial statistical uncertainty. By excluding the data, the CMS prevented an estimated eight percent reduction in pathology reimbursement.
The CMS also finalized a policy to reduce facility practice expense RVUs, but it acknowledged that services billed with the 26-modifier would be exempt from site-of-service payment differentials. As a result, most facility-based pathology services will not face significant reductions. This exemption followed extensive CAP advocacy to urge the CMS to recognize that the proposed differential would have disproportionately harmed pathologists and negatively impacted patient care. The CAP will continue to advocate against reductions to facility practice expense RVUs for services not billed with the 26-modifier, including bone marrow, blood, and apheresis services.
Charles Fiegl is the CAP’s director of communications and media relations.