
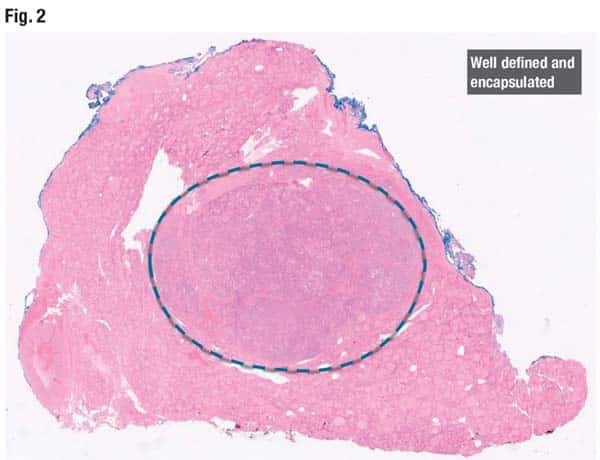
In the periphery of a cross-section of the lobe (Fig. 2) is a normal thyroid gland and variably sized follicles with abundant colloid. In the center is a well-demarcated lesion with a well-defined capsule. No fibrovascular cores are seen.
The most common differential diagnoses for follicular patterned neoplasms of the thyroid include follicular adenoma, follicular variant of papillary thyroid carcinoma (FV-PTC), follicular thyroid carcinoma, and noninvasive follicular thyroid neoplasm with papillary-like nuclear features. “All these lesions, to no surprise, share a relatively similar genetic landscape and all share RAS mutations,” Dr. Dioufa said. Occasionally they can also be seen in association with PAX8/PPARγ rearrangements.
“For this patient, the molecular testing does not help us further refine our diagnosis,” Dr. Dioufa said, “but we go back to our lesion, and we start looking more carefully.” In Fig. 3 is another section of the same lobe. “The capsule is still very well retained and defined, and the pattern remains follicular.” The nuclear features of papillary thyroid carcinoma are identifiable in the right image: nuclear enlargement, clearing of the chromatin, inconspicuous peripherally placed nuclei, and intranuclear grooves.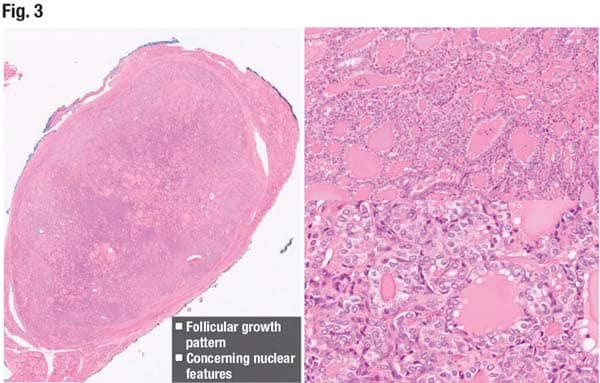
Before 2016, the term for NIFTP lesions was encapsulated FV-PTC.
By architecture, NIFTP should have no more than 30 percent solid, trabecular, or insular growth patterns, and there should be no necrosis and no high mitotic activity (< 3/2 mm2).
Papillae formation is slightly controversial. “In the criteria, we say, ‘no psammoma bodies,’ and we know that psammoma bodies [mean] we are dealing with fibrovascular cores that become avascular and then calcified. This would be a hint that you have some fibrovascular cores and papillae formation in your lesion.”
The well-formed papillae criterion is also slightly controversial. “We can allow some simplified or rudimentary papillary structures present in the lesion, and that is okay, but we should not see well-formed fibrovascular cores lined up with very atypical cells that bear the features of papillary thyroid carcinoma,” Dr. Dioufa said. This stems from the studies in which NIFTP cases were examined retrospectively and the criteria were applied (Nikiforov YE, et al. JAMA Oncol. 2018;4[8]:1125–1126). For the vast majority of the retrospective studies, “we saw that the course was very indolent. However, when we applied the criterion of less than one percent papillary formation, we had some adverse outcomes,” including metastasis to regional lymph nodes in the central compartment, at the time of the surgery or subsequently. These metastatic foci were usually less than 2 mm in size.
Dr. Dioufa’s second case was that of a 56-year-old female found to have two incidental thyroid nodules in the left lobe.
One measured 3.7 cm, had a mixed cystic and solid consistency, and was hypoechoic and lobulated. Immediately adjacent to that nodule was a 1.6-cm nodule that was also solid and hypoechoic. Both were TI-RADS 4, biopsied at an outside institution, and called atypia of undetermined significance (Bethesda category III).
Afirma testing resulted as intermediate risk with NRAS mutations in both nodules, and the patient underwent a left subtotal thyroidectomy. The lesional and normal thyroid tissue is seen in Fig. 12 (right). The morphology of the lesion is identified inside and outside the confines of the tumor capsule (right, bottom).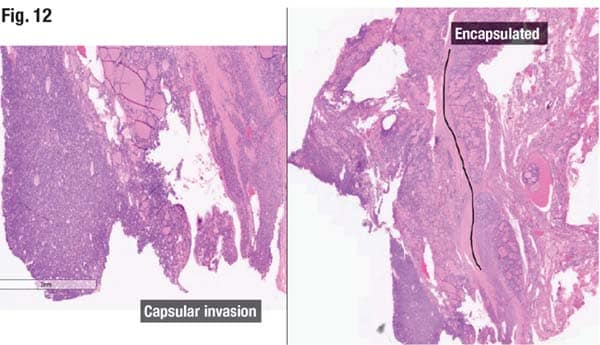
The tumor can be seen (left image) transgressing through the capsule, breaking through to the opposite side. “So you’re dealing with a follicular pattern lesion that is encapsulated and has capsular invasion,” Dr. Dioufa said.
The nuclear features of papillary thyroid carcinoma can be seen in the image on the right in Fig. 13, and the correct classification is follicular variant of papillary thyroid carcinoma.
FV-PTC is composed of small to midsize follicles lined by cells with variable nuclear features of papillary thyroid carcinoma. “We have to be careful because there is a further subdivision in the follicular variants of papillary thyroid carcinoma,” Dr. Dioufa said. The carcinoma identified in the 56-year-old female was an encapsulated FV-PTC because it was partially lined by a capsule—disrupted but present nonetheless.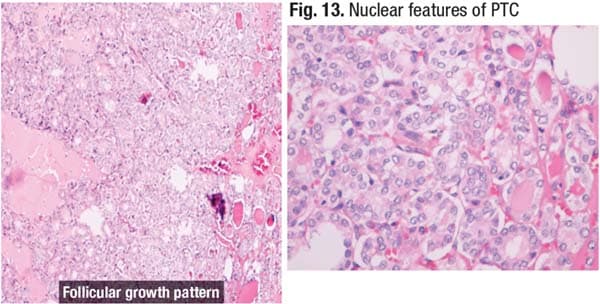
The WHO 2022 definition of encapsulated FV-PTC includes follicular growth pattern (no papillae formation), encapsulation (partial or complete), capsular or vascular invasion, and characteristic nuclear features of PTC. These lesions bear RAS mutations and are biologically, genetically, and clinically closer to the follicular adenoma/carcinoma group. Seen most commonly are distant lung and bone metastases; lymph node metastases are seen less often.
“When we talk about encapsulated follicular variants of PTC, if we have only capsular invasion, this will be a minimally invasive encapsulated follicular variant of papillary thyroid carcinoma,” Dr. Dioufa said. But if there is an angioinvasion, it would be best classified as an encapsulated FV-PTC with angioinvasion.
“Again, angioinvasion and capsular invasion are two things we hunt for,” she said. “It’s important to set these lesions apart because they have the same genetic landscape, mutations, and biologic behavior as the follicular adenoma and follicular carcinoma categories.”
Cytology alone is not always able to correctly classify the lesion, but combining cytology with sonography images, gross examination, and microscopy of the capsular distortion and invasion would better enable correct classification.
In the 2023 Bethesda System for Reporting Thyroid Cytopathology is a group of intermediate-risk lesions that range from more benign to more malignant (Ali SZ, et al. Thyroid. 2023;33[9]:1039–1044). “These lesions have the same cytologic features, the same genetic landscape, and this is why it becomes so challenging for us,” Dr. Dioufa said. “It almost forms a spectrum that requires us to examine carefully and thoroughly the lesion in order to best classify it.”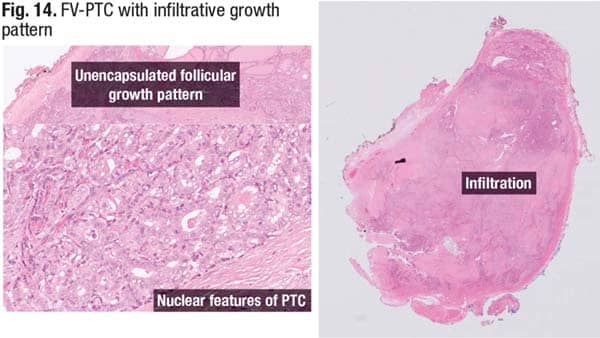
In Fig. 14, there is an infiltrative FV-PTC that is haphazardly arranged and in which no capsule can be identified. On the right is a nest of follicular cells growing haphazardly and infiltrating the surrounding thyroid parenchyma, causing desmoplasia and fibrosis.
“We discriminate between the encapsulated and the infiltrative subtype because these behave differently,” she said, noting they seem to be distinct from a biological standpoint as well. FV-PTC with infiltrative growth pattern has a more frequent incidence of BRAF V600E mutations, increased risk of recurrence, and increased lymph node metastasis.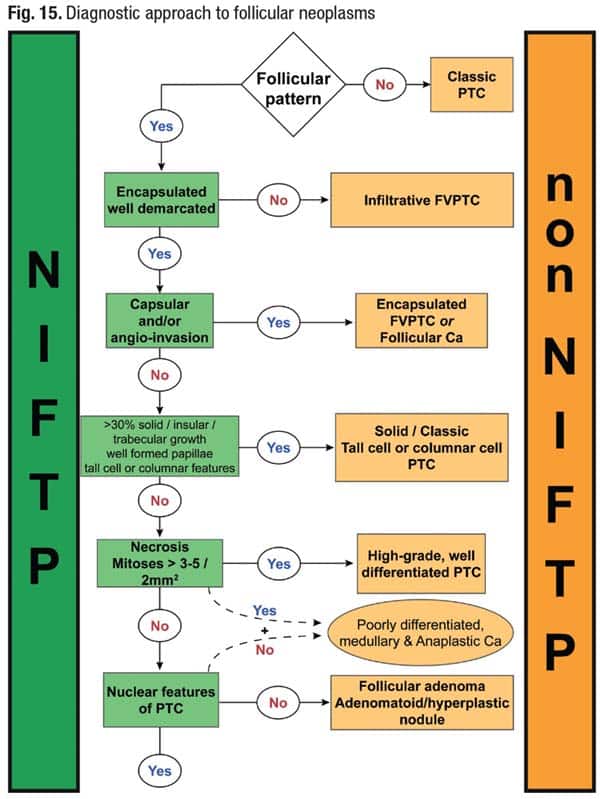
Dr. Dioufa’s algorithm for diagnosing follicular neoplasms is seen in Fig. 15.
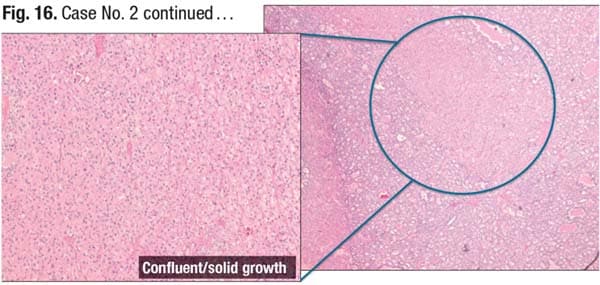 In closing, she returned to case No. 2. Examination of the patient’s second nodule revealed follicular pattern in the periphery of the section (Fig. 16). “However, in the center you have back-to-back follicles,” she said. Solid growth can be seen, and in the right image there is trabecular growth of the follicular cells. When Dr. Dioufa’s team examined additional sections, they saw areas of hyalinization or potential necrosis arising in the center and dropout of follicular cells in the second nodule, raising high suspicion for a higher-grade lesion.
In closing, she returned to case No. 2. Examination of the patient’s second nodule revealed follicular pattern in the periphery of the section (Fig. 16). “However, in the center you have back-to-back follicles,” she said. Solid growth can be seen, and in the right image there is trabecular growth of the follicular cells. When Dr. Dioufa’s team examined additional sections, they saw areas of hyalinization or potential necrosis arising in the center and dropout of follicular cells in the second nodule, raising high suspicion for a higher-grade lesion.
Amy Carpenter is CAP TODAY senior editor.