
From the CAP Cytopathology Committee;
Jordan Paul Reynolds, MD, Derek B. Allison, MD, Editors
Derek B. Allison, MD
Xiaoqi Lin, MD, PhD
January 2025—Renal mass biopsy has become an indispensable pre-management diagnostic tool, especially as incidental renal masses are increasingly detected with modern imaging techniques. It offers the patient the opportunity to get a definitive diagnosis without necessitating nephrectomy, especially helpful for patients with advanced disease or those who are poor surgical candidates. This is crucial, as certain renal cell carcinoma (RCC) subtypes have significantly different prognostic outcomes and therapeutic implications, making it essential to subtype RCCs in addition to distinguishing between benign and malignant lesions. For instance, systemic treatment strategies diverge markedly between clear cell RCC and non-clear cell RCC subtypes, underscoring our role in guiding personalized therapy choices. This article synthesizes key findings and diagnostic challenges most encountered on renal mass biopsy, with a focus on clear cell RCC, clear cell papillary renal cell tumor, TFE3-rearranged RCC, papillary RCC, oncocytoma, and chromophobe RCC.
Key findings and diagnostic challenges
Clear cell renal cell carcinoma. Clear cell RCC is the most prevalent subtype of RCC, characterized by cohesive nests of fairly uniform cells with abundant pale or vacuolated cytoplasm interspersed with stromal components and capillaries. These cells often display frayed cell membranes and round nuclei that are positioned either centrally or eccentrically. As the grade increases, the cytoplasm tends to become more granular or denser while nucleoli become increasingly prominent. Immunohistochemical patterns, such as diffuse boxlike CA9 and vimentin positivity and mostly CK7 negativity, aid in distinguishing clear cell RCC from other RCCs. Occasionally, clear cell RCC may show a focal cuplike CA9 pattern in certain architectural or tangentially sectioned areas, potentially mimicking clear cell papillary renal cell tumor (CCPRCT). Additionally, in cystic clear cell RCCs, CK7 staining can appear in the cystic lining, creating diagnostic ambiguity, as CCPRCT also frequently presents with cystic features and CK7 positivity. In small biopsies where definitive differentiation is challenging, pathologists may use descriptive diagnoses, such as renal cell tumor with clear cell features, accompanied by a diagnostic comment addressing limitations and differential considerations. Molecular tests may help distinguish clear cell RCC from its mimics in biopsy with no definitive morphological or IHC features for clear cell RCC.
Clear cell papillary renal cell tumor (CCPRCT). CCPRCT is generally an indolent tumor, making conservative management a viable option in certain clinical scenarios, particularly if the tumor is small and the patient isn’t a great nephrectomy candidate. Therefore, it is crucial to reserve this diagnosis for cases displaying classic features and unequivocal staining patterns, particularly when working with small biopsy samples. Morphologically, CCPRCT is composed of clear cells arranged in tubular and papillary formations, with eccentric low-grade nuclei oriented toward the lumen or surface of papillae. CCPRCT typically exhibits diffuse CA9 positivity in a cuplike pattern and is diffusely CK7-positive, which aids in distinguishing it from more aggressive RCCs. However, in architecturally complex or tangentially sectioned specimens, CCPRCT may exhibit a boxlike CA9 staining pattern, mimicking the appearance of clear cell RCC. Recognizing these potential variations in staining is essential to avoid misclassification, especially in limited biopsy samples where definitive differentiation can be challenging.
Papillary renal cell carcinoma. Papillary RCC typically displays papillary structures with fibrovascular cores and granular or vacuolated cytoplasm with round nuclei oriented toward the fibrovascular cores; however, the growth pattern can show tubular predominant areas as well as solid sheets. In addition, foamy or hemosiderin-laden macrophages may be present in the background. Although papillary RCC was previously subdivided into types one and two, current World Health Organization guidelines recommend against this subdivision, instead emphasizing broader morphologic and molecular features. Papillary RCC’s CK7 positivity and diffuse and strong AMACR expression help differentiate it from clear cell RCC or CCPRCT, but its potential to present with solid or biphasic patterns in limited biopsy samples can pose diagnostic challenges. Comprehensive morphologic and IHC evaluation is necessary to ensure accurate subtype classification.
TFE3-rearranged renal cell carcinoma (TFE3-rRCC). TFE3-rRCC is a rare yet aggressive subtype of RCC, notable for its morphologic diversity and distinct molecular profile. Cytologically, TFE3-rRCC displays prominent, sometimes eccentric nucleoli, with variably vacuolated, clear, and/or granular eosinophilic cytoplasm (occasionally with hyaline globules) arranged in papillary, nested, or tubular patterns. IHC analysis often includes positive staining for markers such as TFE3 (diffuse and strong), cathepsin K (subset of cases), AMACR, and PAX8, while CA9 is usually negative, helping to distinguish TFE3-rRCC from other RCC subtypes. Given its overlap with CCPRCT and papillary RCC, diagnostic confirmation should follow a sequential approach: morphologic evaluation, IHC panel, and molecular testing, such as FISH or RNA next-generation sequencing, to detect TFE3 rearrangements.
Oncocytoma and chromophobe renal cell carcinoma. Oncocytomas are benign renal neoplasms that can closely resemble other eosinophilic renal tumors, necessitating careful evaluation in renal mass biopsies. Cytologically, oncocytomas are composed of loosely cohesive or dispersed, large, round cells with abundant, granular cytoplasm. The cells typically have centrally placed, round nuclei with smooth nuclear contours, even chromatin, and inconspicuous nucleoli. Oncocytomas are positive for CD117 and generally lack CK7 staining; however, focal CK7 positivity may be observed in areas of central scarring, potentially leading to diagnostic confusion, as CK7 positivity is more typically associated with chromophobe RCC. IHC can help distinguish oncocytoma from low-grade oncocytic tumor, which is negative for CD117 and positive for CK7.
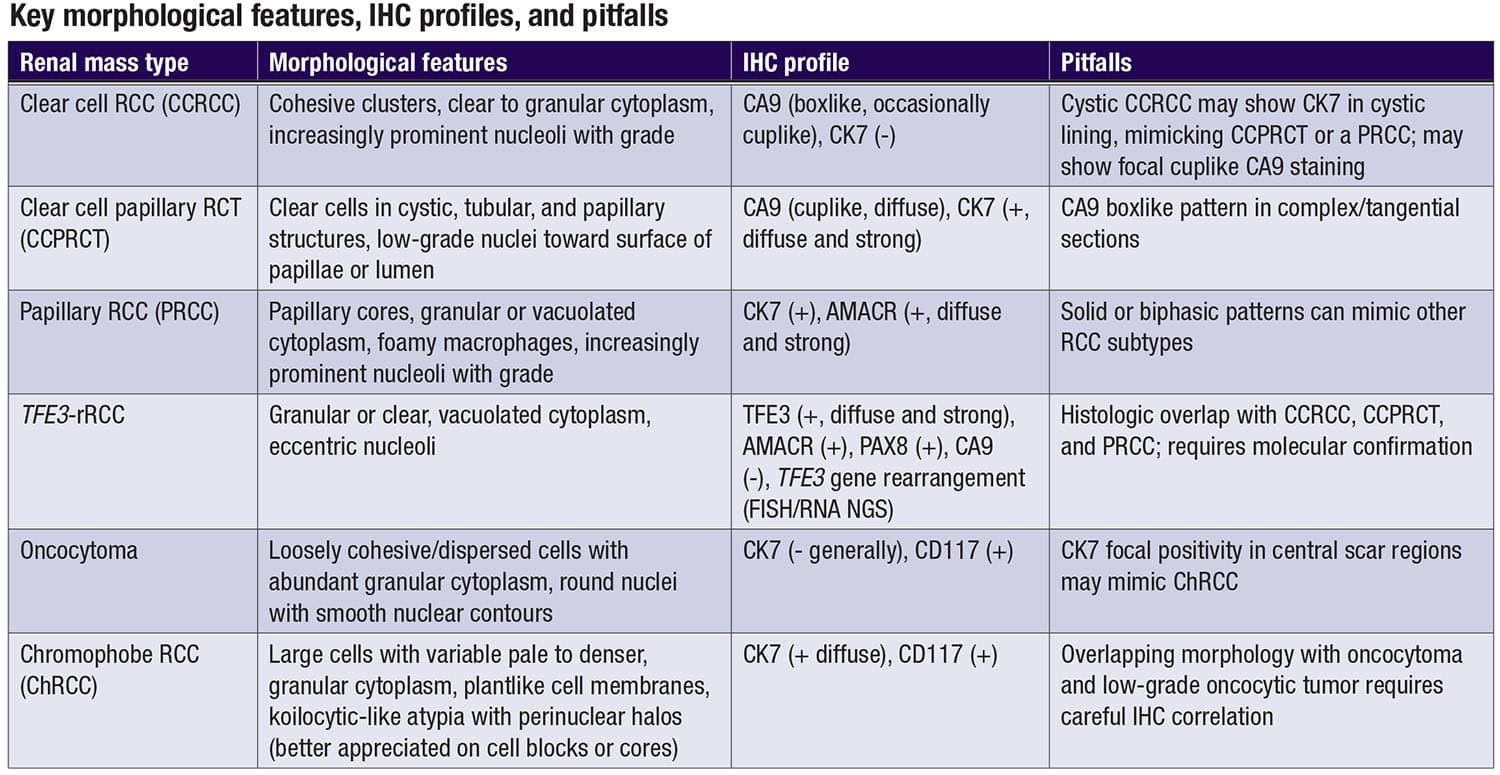 Chromophobe RCC is characterized by sheets of large polygonal cells, some with pale cytoplasm and some smaller cells with denser, granular cytoplasm, distinct cell borders, and prominent perinuclear halos (better appreciated on cell blocks or cores). Nuclear features in chromophobe RCC include irregular shapes, wrinkling, and anisonucleosis. Unlike oncocytoma, CK7 positivity in chromophobe RCC is typically diffuse and intense, aiding in differentiation, while CD117 is positive in both. This variability in CK7 staining across oncocytomas and chromophobe RCC highlights the importance of correlating morphology with IHC findings to ensure accurate diagnosis and avoid potential misclassification. CD117 positivity can help distinguish chromophobe RCC from its mimic, low-grade oncocytic tumor.
Chromophobe RCC is characterized by sheets of large polygonal cells, some with pale cytoplasm and some smaller cells with denser, granular cytoplasm, distinct cell borders, and prominent perinuclear halos (better appreciated on cell blocks or cores). Nuclear features in chromophobe RCC include irregular shapes, wrinkling, and anisonucleosis. Unlike oncocytoma, CK7 positivity in chromophobe RCC is typically diffuse and intense, aiding in differentiation, while CD117 is positive in both. This variability in CK7 staining across oncocytomas and chromophobe RCC highlights the importance of correlating morphology with IHC findings to ensure accurate diagnosis and avoid potential misclassification. CD117 positivity can help distinguish chromophobe RCC from its mimic, low-grade oncocytic tumor.
Clinical relevance
The precise classification of renal neoplasms has direct implications for clinical management. Clear cell RCC benefits from a range of FDA-approved therapies, including tyrosine kinase inhibitors like sunitinib and pazopanib, immune checkpoint inhibitors such as nivolumab, and combination therapies that target VEGF and PD-1 pathways. In contrast, non-clear cell RCC subtypes have fewer targeted treatment options, with many relying on off-label use of agents approved for clear cell RCC. Recently, MET inhibitors, such as savolitinib, have shown efficacy in MET-driven papillary RCC, marking progress in personalized treatment for non-clear cell RCC subtypes. Furthermore, there are a number of clinical trials available for non-clear cell RCCs for which the patient may be eligible if a specific diagnosis can be made. Active surveillance and ablation have been implemented in management of benign renal neoplasm or small low-grade renal cell carcinoma that need definitive pre-management diagnosis. These therapeutic distinctions underscore the need for an accurate renal mass biopsy diagnosis, as they allow for tailored treatment that optimizes outcomes and reduces unnecessary intervention.
Conclusion
The interpretation of renal mass biopsy, even in routine cases, requires a detailed approach that combines morphology and IHC, as well as molecular diagnostics when necessary. Understanding the variability in staining patterns, such as focal CA9 cuplike patterns in clear cell RCC and CK7 positivity in cystic areas in clear cell RCC or central scarring in oncocytoma, is essential for avoiding diagnostic pitfalls. These insights enable us to provide precise and actionable diagnoses, ensuring patients receive individualized management strategies that align with their tumor’s specific characteristics.
Dr. Allison is associate professor of pathology and urology and vice chair for research, University of Kentucky College of Medicine, Lexington. Dr. Lin is professor of pathology (cytopathology and thoracic pathology), Northwestern University Feinberg School of Medicine, Chicago. Both are members of the CAP Cytopathology Committee.