
Amy Carpenter
December 2025—A clinical decision support solution to over- or misordered CBC and differential tests was found to work and be sustainable across seven hospitals in a system—and could be applicable in others.
It began in 2022 at Massachusetts General Hospital, which, like other laboratories during the pandemic, was short staffed. At MGH, highly trained hematology clinical laboratory scientists needed for complex manual differentials were in short supply. “This was an area of particular need,” said Grace Mahowald, MD, PhD, informatician and director of the MGH core laboratory, in an ADLM session in July.
Of the top daily laboratory tests ordered at MGH, of which the CBC and CBC/diff were No. 1, all are considered low cost per test and have a low labor requirement per test, she noted. “Even the CBC and diff, when done by auto-diff, is a fairly low labor test. You just load it on and off it goes.”
But the manual differential can be labor-intensive, and 16 percent of the CBC and differentials performed at MGH were requiring a manual differential. Among inpatients, it was 25 percent, and overall two-thirds of manual differentials were performed on inpatients. Complex manual differentials can require more than 30 minutes of technologist time. “So this is a significant problem in our view,” she said.
Dr. Mahowald and colleagues studied all recurring inpatient orders for the CBC and differential and found the most problematic to be those ordered more than once a day (four percent of monthly inpatient orders). “It looked like they were almost entirely from bleeding patients where the differential isn’t needed,” Dr. Mahowald said.
Daily orders made up 56 percent of the monthly inpatient recurring orders for the CBC and differential. “You could argue there are some clinical situations where you might need a daily diff,” she said. “But in talking with many of our clinicians from medicine and oncology, [we] found they universally agreed daily was not necessary.”
The CBC and differentials ordered “as needed” accounted for 27 percent monthly. Some units prefer CBC and diffs as needed, she said, “but we didn’t feel a CBC and diff as needed was the right order.” When a patient begins to bleed, a CBC may be needed but not a CBC and differential.
Dr. Mahowald and colleagues took steps to evaluate how well an alert would work in targeting CBC and differential orders placed daily, greater than once daily, or as needed.
In designing their clinical decision support intervention for inpatient orders, they chose a soft stop, which is an interruptive alert. “It’ll pop up, but you can click through to bypass,” Dr. Mahowald said.
A hard stop prevents ordering but was judged to be infeasible because there are reasonable indications. Another CDS option, “an order question, requires you to put in a reason, but it’s often not as easy to monitor,” she said, and may be a weaker interruption than a pop- up—“it’s easy to pick a choice, and probably the first one, and move on.” Instructions within the order window are not necessarily visible to providers and unlikely to be read, and provider education cannot reach everyone, though “it’s something you have to do in conjunction with your alert.”
Dr. Mahowald lists the questions that come up as an alert is being built. First, how many alerts are needed? She and her colleagues went with three different alerts with three custom messages to target the daily, more than daily, and as-needed CBC and differential orders.
The alerts say that in most situations a daily CBC and differential is not clinically indicated but that it would be reasonable to get a daily CBC or a CBC and differential once or every other day. A popular option at MGH is a custom package: a CBC and differential every other day (starting that day), alternating with a CBC every other day (starting the next day).
Providers who order a CBC and differential more than once a day see this message: “CBC (without differential) should be used for patients with bleeding or another need to monitor cell counts more than once daily.” The alternative orders presented in the alert are targeted toward situations in which the patient is likely bleeding.
For the as-needed situation, too, the aim is to steer the orderer to the CBC instead of the CBC and differential.
Second, what action should trigger the alert? Each CBC and differential order has a rule for the frequency that can trigger the alert (Fig. 1).
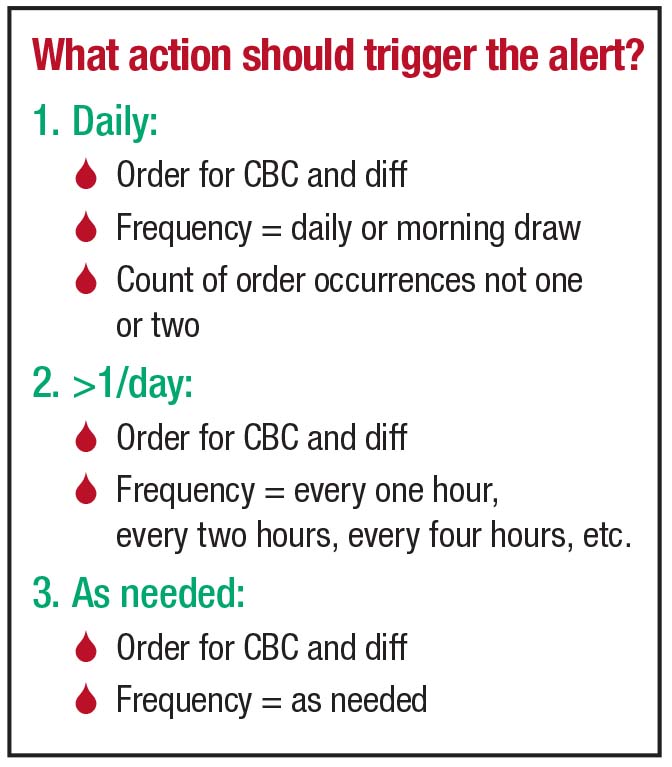
Third, what is the target patient population? “We’re targeting inpatients because we’re talking about daily labs,” Dr. Mahowald said. After talking to many providers, the only patients the laboratory decided to exclude from the alert were oncology and active transplant patients and patients enrolled in a research study. Providers with patients who meet one of these criteria are not shown the alert and can order their daily CBC and differential.
Fourth, who are the target providers? “We didn’t put any restrictions on this,” she said. “All providers, anyone who is ordering a CBC and differential, are eligible to see the alert.” The aforementioned specific patient exclusions would still apply.
And when should the alert be shown? The four options are when the patient’s chart is opened, when the orders activity is opened, when the order is selected, or when the order is signed. For this situation, the fourth option is best, Dr. Mahowald said, because the frequency is not known until the order is being signed.
With any alert, providers should be given reasons they can choose from for not following the advice in the alert, Dr. Mahowald said. They can be as generic as “clinically indicated.” She and colleagues thought monitoring the absolute neutrophil count was a reasonable option for needing a differential. The last reason to select is “other,” with a required comment.
MGH’s interruptive alert for CBC and differential orders placed daily (Fig. 2) carries a message that says in most situations, a daily CBC and differential is not clinically indicated. It then says that a CBC (without differential) should be used for patients with bleeding or another need to monitor cell counts daily. If a CBC and differential is needed, it says, consider changing the frequency to once or every other day. Clicking the accept button on the bottom of the alert will by default remove the CBC and differential order, Dr. Mahowald said. If the provider clicks to “remove” the CBC and differential order, four alternative order options are available: CBC (daily), CBC and diff (once), CBC and diff (every other day), and CBC and diff (every other day, starting now) plus CBC (every other day, starting tomorrow).
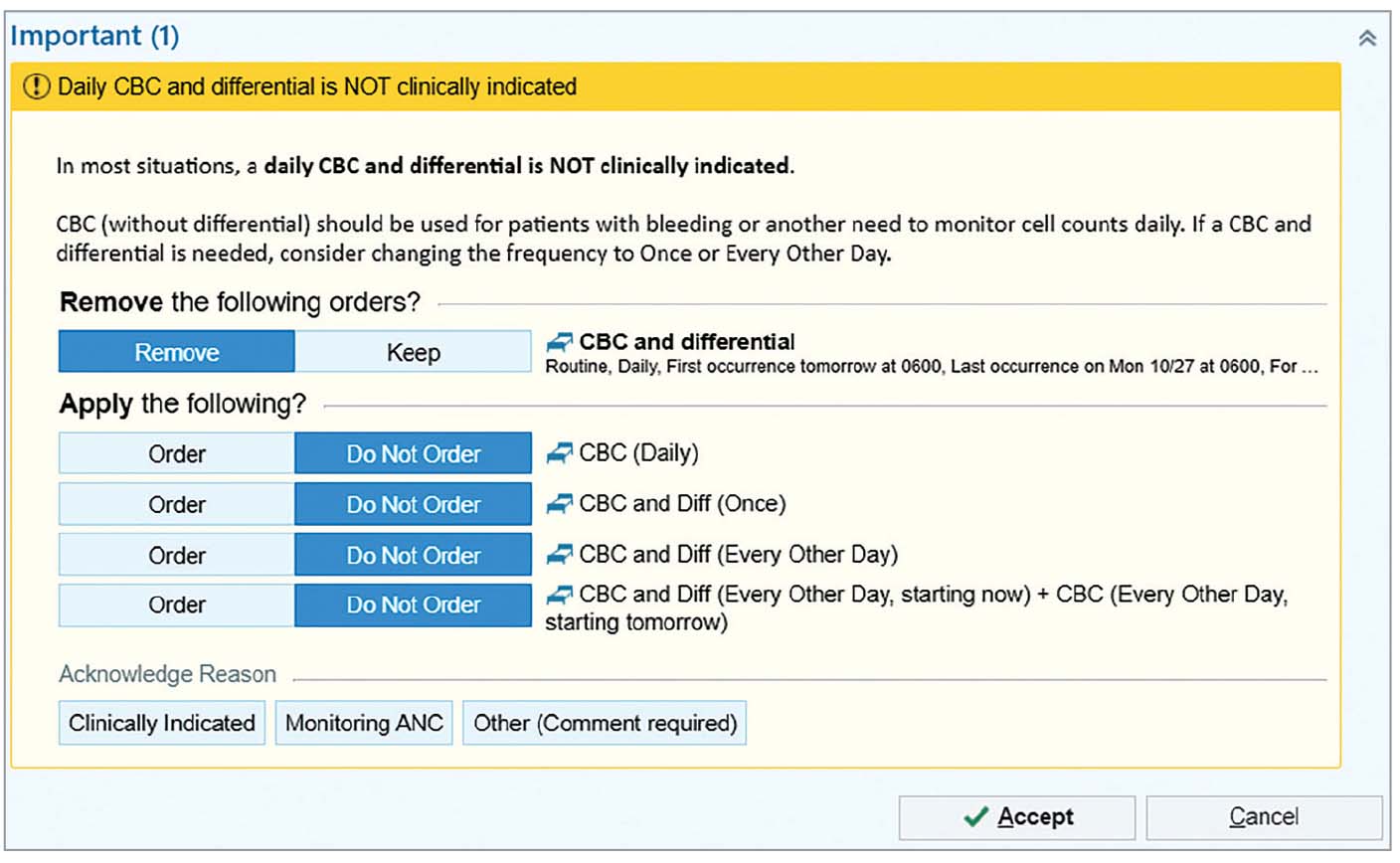
“We couldn’t pre-choose one of these alternative orders for them because we can’t completely read their minds as to what they want,” she said. “But I’d say a lot of people take the opportunity to choose a simple substitution for what it is that they want and move on.”
With a new alert, step No. 1 is to run it silently in the background to ensure it fires appropriately and doesn’t target the wrong people, she said, in this case oncology patients and others.
Communicate with frequent users. “Ideally, this should happen during the design process or even before.” And measure success, she said, which can consist of a reduction in differentials, a study of turnaround time, and the alert acceptance rate. “If all are successful, you can plan to expand the intervention to other sites.”
The alerts were implemented at MGH in July 2022.
Overall test volume for CBC and diff decreased by 32 percent post-implementation, with a corresponding decrease of 22 percent in manual differentials performed. “Not surprisingly, there was a corresponding increase in the volume of CBC tests for all three frequencies,” Dr. Mahowald said. Turnaround time for manual differentials declined by a mean of 41.5 minutes, with a mean decrease of up to 90 minutes during peak morning hours.
In the one-year post-implementation period, the alert acceptance rates were found to be 33 percent for the daily order frequency, 55 percent for more than once daily ordering, and 45 percent for as-needed ordering.
The alerts used at MGH were implemented in the other Mass General Brigham hospitals—a second academic center and five community hospitals—between August and October 2022, with declines at each site of nine percent to 54 percent post-implementation and a corresponding increase in CBC volume. No negative feedback was received from any of the seven sites.
Dr. Mahowald and colleagues expanded on this work in a 2024 article (Mahowald GK, et al. Am J Clin Pathol. 2024;162[2]:151–159), in which they made the following points:
- By not repeating manual differentials in short intervals where meaningful differences were unlikely, the laboratory was able to focus resources on differentials more likely to have a clinical impact. “At a single hospital,” they write, “the observed reduction of a mean of 898 differentials per month is estimated to free 2694 hours of technologist time per year (assuming a mean of 15 minutes for each manual differential), effectively saving a full-time technologist that can be redeployed to better support clinical care.”
- Estimating an incremental cost of $0.34 per WBC differential, the cost savings to convert 5,257 CBC diffs per month to CBC is $21,449 per year at one site and $52,708 (for 155,024 CBC diffs) per year across the health care system.
- The faster turnaround time for manual differentials may shorten length of stay for patients for whom the differential results may be needed for discharge planning.
- The number of times the alert has fired has declined over time. The alert for order frequencies of greater than once daily fired 164 times in the first full month post-implementation but decreased to 59 the next month and remained at a mean of 56 per month after the first month. Similarly, the number of alerts for daily CBC and differential orders dropped from 1,001 to a mean of 612 per month. “This suggests,” the authors write, “that providers have learned from the alert to place fewer orders at these order frequencies and that this may be the major mechanism by which the number of orders has decreased.”
- The seven hospitals in the Mass General Brigham system span a variety of patient care settings, suggesting the clinical decision support they describe in their article “would likely be widely applicable across many laboratories and hospital systems,” the authors write. And in light of the consistent effect they observed, they write that the “savings of labor and reagents would be significant at a national level given the magnitude of the effect and the generalizability.”
Amy Carpenter is CAP TODAY senior editor.