
Khosrow Shotorbani, MBA, MLS (ASCP); Kathleen Swanson, MS, RPh; Bruce A. Friedman, MD; Eric F. Glassy, MD; Michael J. Crossey, MD; Mark K. Fung, MD, PhD; Karen L. Kaul, MD, PhD; Octavia M. Peck Palmer, PhD; Nancy Stratton, MBA; Myra L. Wilkerson, MD; Richard J. Zarbo, MD, DMD; Gaurav Sharma, MD; Ronald Jackups Jr., MD, PhD; Ulysses G.J. Balis, MD; Junya Fukuoka, MD, PhD; John V. Groth, MD; Lena Chaihorsky; Merce Jorda, MD, PhD, MBA; Chen Liu, MD, PhD; Mario Plebani, MD; R. Keith Laughman, DBA; James M. Crawford, MD, PhD
April 2025—Many look to CAP TODAY to be a central disseminator of news, opinion, and other important information, and it has in the past filled that role in response to others’ requests. One such recent request is that of the Clinical Lab 2.0 movement, established in 2017 by the Project Santa Fe Foundation. We present here, for CAP TODAY readers, the Clinical Lab 2.0 movement’s position paper. We welcome feedback.
The views expressed here are not necessarily those of CAP TODAY or the College of American Pathologists.
“As is our pathology so is our practice: what the pathologist thinks today the physician does tomorrow.” —Sir William Osler, British Medical Journal, July 24, 1909; 2534:185–189.
“Insanity is doing the same thing over and over again and expecting different results.” —Rita Mae Brown, Sudden Death, 1983 (not Albert Einstein, as is popularly thought).
The transition to value-based health care, emphasizing quality outcomes over service volume, presents challenges and opportunities for pathologists and clinical laboratorians.
To remain relevant in this evolving landscape, lab professionals must adapt their roles and focus on delivering value. Others are seizing this opportunity. Laboratories risk being left not as an asset for driving the delivery of high-quality, cost-effective health care, but as a commodity supplier focusing only on lowest cost for a resulted test. We must emphasize that our use of the term “clinical laboratory” is inclusive of laboratory medicine, anatomic pathology, molecular pathology, pathology informatics, and the broad intersection of these domains.
We argue that a new role for pathologists and the clinical laboratory, along with a new business model to pay for this role, is not only possible but essential to survival. If value-based care is the future, what can pathologists bring to that future? Can pathologists and the clinical laboratory serve as a linchpin in driving improved patient and population outcomes? Can pathologists and the clinical laboratory, as the first to know the diagnostic information they provide, be responsible for triggering coordinated care pathways for the patient’s health care journey? Will pathologists provide leadership for the multidisciplinary and interprofessional programmatic delivery of health care? We believe that the answer to all of these questions is yes. After examining the current market dynamics of value-based care, we will explore each of these questions in turn.
Value-based care and clinical laboratories: an inflection point
In the book Only the Paranoid Survive: How to Exploit the Crisis Points That Challenge Every Company, Andrew Grove defines a “strategic inflection point” as a major change in the competitive environment that requires a fundamental change in business strategy. Depending on how organizations adapt to the change, they can either grow or suffer decline.1 The evolving landscape of U.S. health care has brought the laboratory industry to its own inflection point.
In 2011, 11 percent of health care payments were tied to quality and value. By 2020, that number had grown to 60 percent.2 While the transition from a fee-for-service economy to one that ties payments to quality and value may seem remote to the practice of pathology and laboratory medicine, it is critical to recognize that diagnostic intelligence and process design is central to value-based care, which rewards early diagnosis and intervention, and the optimized use of health care resources. While the actual performance of laboratory testing is being progressively devalued, the optimization of patient care on the basis of that testing is being assigned greater and greater value. This dichotomy is central to the arguments made in this treatise.
To wit: The 2023 report of the Healthcare Payment Learning and Action Network (HPLAN) found that 24.5 percent of all health care payments (commercial and government) were already in a two-sided risk model—both “upside” and “downside.”3 This migration toward risk-based payments is in alignment with the goal of the U.S. Centers for Medicare and Medicaid Services to have all of Medicare and the greater part of Medicaid beneficiaries enrolled in Accountable Care benefits programs by 2030.4 Payers also recognize the trend in alternative payment models, with 73 percent believing these models will continue to rise.3
From the provider perspective, while there are growing pains in the primary care community as fee-for-service transitions to value-based payments,5 Medicare’s value-based care models have seen a 25 percent increase in health care provider participation from 2023 to 2024 alone, based on data from the CMS.6 Additionally, 11,000 Americans turn 65 each day and become eligible for Medicare, and the Congressional Budget Office projects that Medicare enrollment will rise from 60 million in 2023 to 74 million in 2034. Both points emphasize the importance of providers becoming proficient in managing Medicare-enrolled patients under value-based benefits plans.
Additional major changes already impacting the laboratory in today’s health care market include the following:
- Significant financial reductions in clinical laboratory reimbursements due to the Protecting Access to Medicare Act (PAMA) of 2014.
- Bundled Diagnosis-Related Group (DRG)-like payments on capitated per patient per month models more than likely impacting surgical procedure pathology payments (e.g. for Current Procedural Technology codes 88305, 88307, and 88309).
- Shrinking markets available to independent laboratories, owing to increased physician employment by integrated delivery networks, bringing physician practice laboratory work under preexisting relationships with other clinical laboratories.
For laboratories within integrated delivery networks and hence part of the integrated health system budgeting process, health system leaders increasingly view the clinical laboratory as unable to deliver positive margins from the fee-for-service market, and with steadily decreasing monetizable value as a system asset. In-system laboratories are thus at risk of full or partial divestment to commercial laboratories, disempowering the in-system laboratory from being an active player in health system strategic initiatives. Conversely, independent laboratories that depend on fee-for-service for their financial viability face their own financial reckoning under downward pressure on revenues. To the extent that both in-system and independent clinical laboratories base their financial future on “doing the same thing over and over again” (fee-for-service), our version of potential insanity is expecting this business model to sustain our future. This assumption may no longer be true. The result will be different, especially since fee-for-service does not provide funds flow for value-based activities. The business model that is value-based care must now be part of our collective “tomorrow.”
What do pathologists and the clinical laboratory bring to value-based care?
The asset that the clinical laboratory brings to the table is the structured local data that informs the delivery of both patient-centered health care and regional population health. The asset that pathologists and board-certified clinical PhDs bring is profound and deep expertise in the medical science of human disease. Along with the administrative managers of the clinical laboratory, we bring extensive knowledge and experience in strategic planning and tactical operations to bear on the creation of coordinated care programming for a regional population. We also recognize doctorates in clinical laboratory science (DCLS) as high-complexity laboratory directors and contributors to the goals of value-based care.
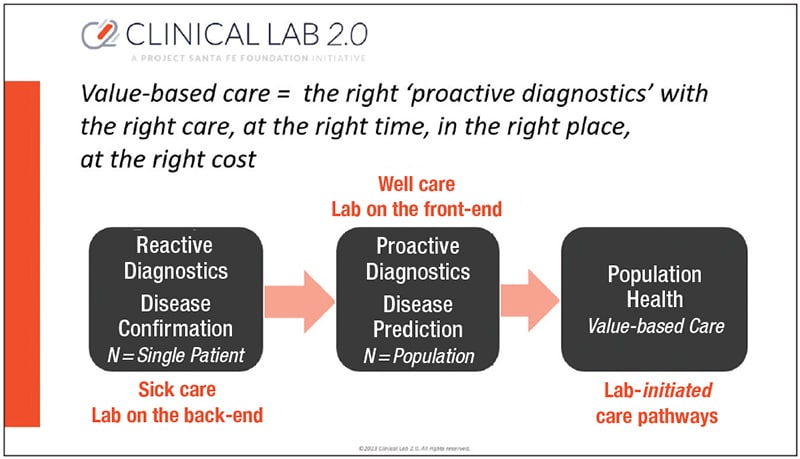
The fundamental pivot that pathologists and clinical laboratories must make to realize the value of our asset, is: 1) to be active members of the multidisciplinary and interprofessional teams that are designing and delivering the integrated care required for risk-based and value-based care (two arms of the same system),7 and 2) to be the experts to interpret and make actionable the data that our clinical laboratories generate. The actions must be in the health care delivery space of risk stratification, wellness care and prevention, early detection and intervention, and ultimately patient-centered coordinated care, with attendant avoidance of downstream health care costs.8 The intersection of the laboratory practice and value-based care can be visualized in Fig. 1. The laboratory’s shift from a reactive approach (subject entirely to receipt of test samples from physician-ordered clinical workflow) to a proactive approach (being part of the team for clinical management, inclusive of when to perform testing, on what samples, and on which patients) empowers laboratories to be active contributors to population health management. This shift supports value-based care, defined by the CMS as focusing on the quality of care, provider performance, and the patient experience.9
Can pathologists and the clinical laboratory serve as the linchpin in value-based care?
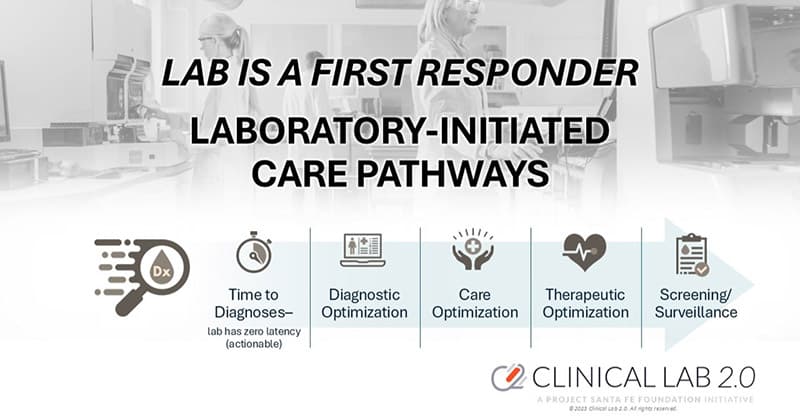
Reach: Clinical labs and pathology touch more lives than any other sector in health care. Each interaction generates structured data that influences a substantial majority of clinical decisions (whether 70 percent or otherwise).10 Being among the “first to know” about the onset of a health condition, clinical labs can act as frontline first responders in patient care (Fig. 2). Indeed, one can argue that, having provided clinically actionable information for the management of a patient, the laboratory carries a moral responsibility to ensure that information is acted upon. While the laboratory cannot do so for the millions of patients it touches in any given year, that moral responsibility can be discharged by providing leadership in ensuring that clinical programming delivers effective health care to the regional population served by that laboratory.
Cost-effectiveness: One can also argue that the clinical laboratory is the most cost-effective source of information for management of a population. It touches virtually every patient receiving health care. Innovation and programmatic initiatives involving laboratory services can be propagated broadly through a health system owing to the high level of integration and standardization that are an essential part of laboratory operations. Perhaps most importantly, both at the individual patient and at the programmatic level, pathologists and clinical PhDs are highly knowledgeable experts in the meaning and impact of their informational product. The opening quote of Sir William Osler rings true well over a century later.
Zero latency: The information emanating from the clinical laboratory is part of the clinical workflow: There is zero latency. A resulted test (whether anatomic pathology or laboratory medicine) can be acted upon immediately. It is from this wellspring that laboratory leadership begins: Diagnostic optimization can then lead to therapeutic optimization, with the clinical laboratory being an essential partner to the patient and provider in monitoring the success of treatment outcomes.
Real-time clinical surveillance: For the regional population, clinical laboratories serve as real-time surveillance systems for clinical conditions and population health. By continuously monitoring their own data, clinical laboratories can identify trends and patterns that indicate the onset or progression of diseases within the population. In partnership with the population health initiatives of a health system, this proactive approach empowers early intervention and management of patients with or at risk for disease conditions, leading to improved patient and population outcomes.