
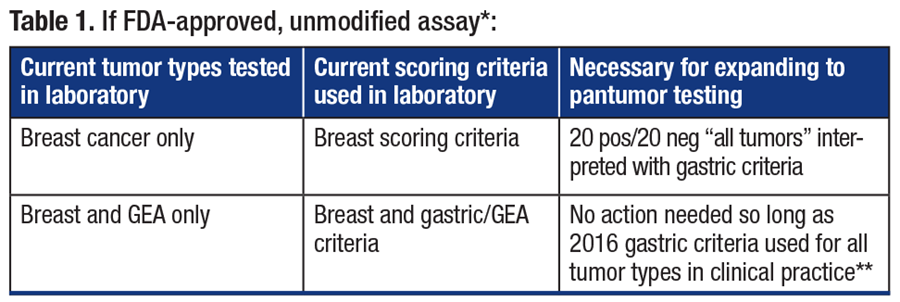
If the laboratory did not previously validate gastric/GEA tumors using the 2016 gastric scoring criteria3 but now is looking to expand beyond breast-only testing, an additional 20 positive and 20 negative tumors representative of tumor types on which gastric scoring criteria are now used (e.g. pantumor, which will include gastric/GEA tumors) is appropriate (Table 1).
**If other interpretation criteria are used (e.g. endometrial serous criteria), then 20 positive and 20 negative cases using these scoring criteria are required.
If a laboratory is performing a modified FDA-approved or an LDT HER2 IHC test, the same guidance applies, but attention to whether more than 20 positive and 20 negative cases are required is left to the judgment of the laboratory/medical director.
Lastly, if a laboratory has never performed HER2 IHC before but now finds conditions necessitate validating an in-house assay, during validation planning the laboratory will need to specify the intended uses, including how many scoring systems are expected to be used in reporting results. If the laboratory intends to offer only one HER2 IHC assay, then the number of “validations” (e.g. 20 positive and 20 negative cases) is equal to the number of intended scoring systems. It would be expected that the validation case set would be representative, but not necessarily inclusive, of all tumor types typically received by the laboratory.
If availability of cases is challenging in a laboratory’s archival materials, participation in the CAP’s Gastric HER2 proficiency testing is a way to accrue cases for assay-scoring system validation for gastric/GEA criteria. If pathologists are interested in additional opportunities to compare performance in interpretation of HER2 across tumor types, a new educational offering from the CAP in 2026 is the opportunity to participate in the Gastric Pantumor, HER2 (GPH) interpretation only educational program.
- Oaknin A, Lee JY, Makker V, et al. Efficacy of trastuzumab deruxtecan in HER2-expressing solid tumors by enrollment HER2 IHC status: post hoc analysis of DESTINY-PanTumor02. Adv Ther. 2024;41(11):4125–4139.
- Goldsmith JD, Troxell ML, Roy-Chowdhuri S, et al. Principles of analytic validation of immunohistochemical assays: guideline update. Arch Pathol Lab Med. 2024;148(6):e111–e153.
- Bartley AN, Washington MK, Ventura CB, et al. HER2 testing and clinical decision making in gastroesophageal adenocarcinoma: guideline from the College of American Pathologists, American Society for Clinical Pathology, and American Society of Clinical Oncology. Arch Pathol Lab Med. 2016;140(12):1345–1363.
- Wolff AC, Somerfield MR, Dowsett M, et al. Human epidermal growth factor receptor 2 testing in breast cancer: ASCO–College of American Pathologists guideline update. J Clin Oncol. 2023;41(22):3867–3872.
Dr. Meserve is vice chair and Dr. Zhang is a member of the CAP Immunohistochemistry Committee. This article was written on behalf of the Immunohistochemistry Committee. Dr. Meserve is chief of the Division of Anatomic Pathology, Maine Medical Center, and technical director of histology and immunohistochemistry at NorDx Laboratories in Maine. Dr. Zhang is professor of pathology and director of gastrointestinal and liver pathology, Department of Pathology, Yale School of Medicine.