
Cytopathology in focus
Christopher O’Conor, MD, PhD
Poornima Hegde, MD
Jordan Reynolds, MD
May 2026—The Papanicolaou test has been a model for cancer screening and prevention since its introduction well over half a century ago. Despite the evolution and innovations in HPV vaccination, testing methodologies, reporting systems, and treatment algorithms, cervicovaginal and lower genital tract cytology continues to be a workhorse for providers and laboratories. Test performance is heavily reliant on specimen quality, and this is no less true for cervicovaginal cytology. The laboratory plays a critical role in the care of patients when it can contribute to avoiding inadequate samples as much as possible. Here we will review the definitions and causes of inadequate Pap smears as defined in the Bethesda System and the remedies to improve adequacy and diagnostic performance.

Test input quality is a critically important yet often overlooked component of quality assurance. The most recent and third edition of the Bethesda System included updates to the definition of cervicovaginal specimen adequacy. An adequate cervicovaginal Pap is defined as follows: 1) a specimen with any abnormal cellular component (including atypical squamous cells of undetermined significance and atypical glandular cells) (Table 1), or 2) a specimen that reaches a minimum cellularity threshold depending on preparation type (8,000–12,000 well-visualized/well-preserved squamous and/or metaplastic cells for conventional cervical specimens and 5,000 well-visualized/well-preserved squamous and/or metaplastic cells for liquid-based preparations). Endocervical cells do not count toward cellularity thresholds, and normal-appearing endometrial cells on their own, regardless of age, do not make a specimen adequate.
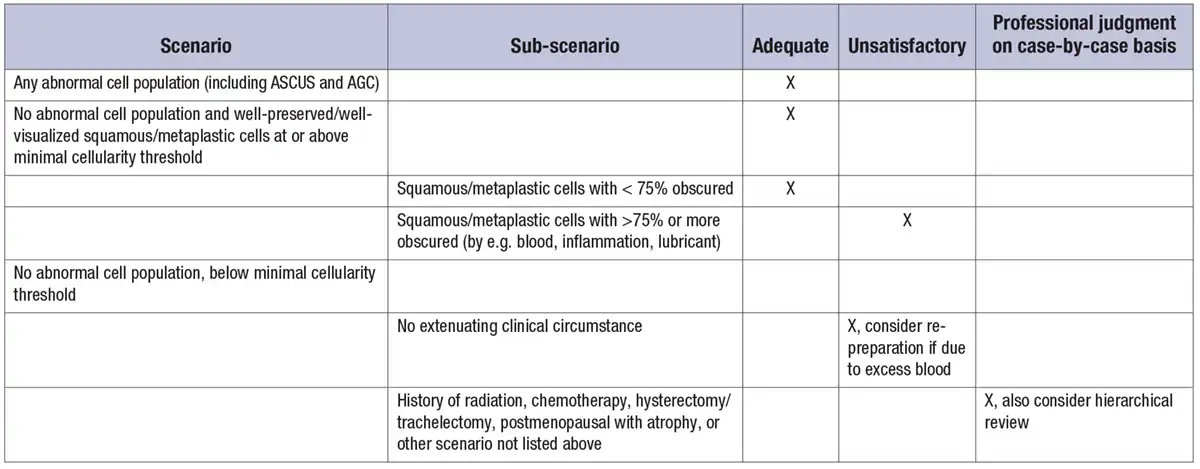
Several caveats to the cellularity thresholds also exist. Specimens with greater than 75 percent of squamous/metaplastic cells not well visualized due to obscuring factors should be deemed inadequate. In addition, given the lack of evidence for the above cellularity thresholds in the following scenarios, a lower threshold for adequacy can be considered at the pathologist’s discretion: history of radiation, chemotherapy, hysterectomy or trachelectomy, or postmenopausal with atrophic changes. Laboratories are encouraged to apply professional judgment and consider hierarchical review when evaluating borderline cases or scenarios not listed above. Any specimen with fewer than 2,000 cells should be unsatisfactory in most cases.