
Anne Ford
April 2018—In analyzing cervical tissue, adjunctive use of p16 IHC with H&E-stained slides improves accuracy and sensitivity, according to the results of the Cervical Tissue Adjunctive Analysis study presented by Thomas C. Wright Jr., MD, in a webinar hosted by CAP TODAY and made possible by an educational grant from Roche Diagnostics.
Dr. Wright, professor emeritus of pathology and cell biology at Columbia University, said p16 staining in the study, known as the CERTAIN study, improved pathologist correlation with a panel of expert diagnoses. “It’s something which, in my opinion, is dramatically changing our ability as pathologists to make the correct diagnosis,” he said.
P16 is a cyclin-dependent kinase inhibitor that is involved in the normal cell cycle. “Under normal conditions, when we get release of E2F from the retinoblastoma gene product, the result is cell cycle progression,” he said. “This also gives us very low-level expression of p16 within the cervical epithelium, low enough expression that you cannot see it with routine immunohistochemistry.”
That overexpression of p16 results in a feedback rebinding of E2F to the retinoblastoma gene product, leading back into cell cycle arrest. “So p16 plays a critical role in the normal cell cycle,” he said. “This allows us to cycle between progression and proliferation and cell cycle arrest. In contrast to the normal cell cycle, when we have a transforming HPV infection or oncogenesis of the cervical epithelium, what we know is that E2F is permanently released from the retinoblastoma gene product by binding of the E7 protein of a high-risk HPV. This leads to cell cycle proliferation. We end up with overexpression of p16. We get genetic instability. And the amount of p16, which is expressed now in the deregulated epithelium, is enough that you can identify it by routine immunohistochemistry.”
For more than a decade, studies have demonstrated the clinical utility of staining cervical epithelium with p16, with a strong correlation between p16 staining and a consensus histology diagnosis of HSIL (CIN 2, 3). It’s only more recently that p16 staining has been shown to improve the reproducibility rate of cervical disease diagnosis. “And when we talk about p16 immunostaining, it’s important that we recognize that it’s just not any staining of the epithelium,” Dr. Wright cautioned. “It is a very specific pattern of staining of the epithelium, which is associated with the presence of a CIN 2, 3 lesion. What we want to see is diffuse strong, what we call block positive, staining of both the basal and parabasal cells in the epithelium. . . . We want to see one-third of the epithelial thickness stained by p16 in order to call it positive staining.”
So how strong is this association? Dr. Wright pointed to a 2010 study in which 1,500 adjudicated cervical biopsies were stained with p16 (Galgano MT, et al. Am J Surg Pathol. 2010;34[8]:1077–1087). Ninety-nine percent of the adjudicated CIN 3 diagnoses stained with p16. For CIN 2 lesions, it was 77 percent. Thirty-nine percent of CIN 1 lesions were p16 positive. Only five percent of normal biopsies were p16 positive. “Clearly what this says is that if you’re positive, you’re unlikely to be a normal biopsy. And if you’re CIN 3, almost inevitably you’re going to be p16 positive. And finally—I can’t stress this enough—39 percent of the CIN 1 lesions were p16 positive. So if something looks like a CIN 1, you call it a CIN 1, even if it’s p16 positive.”
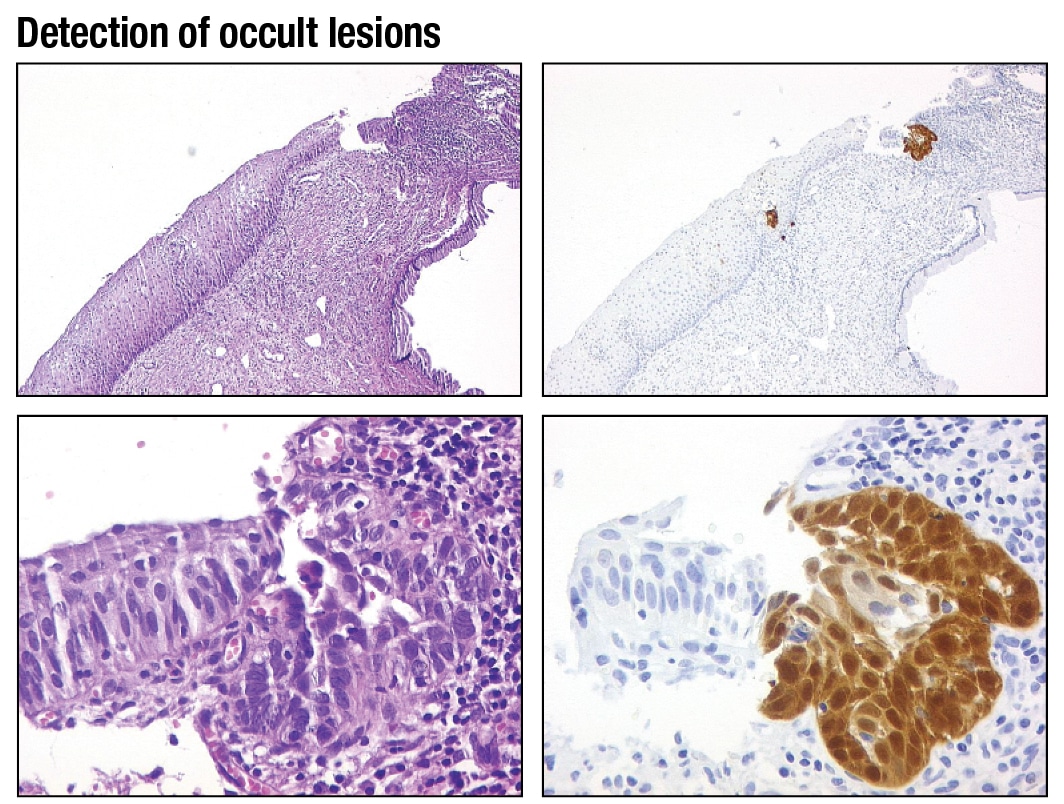
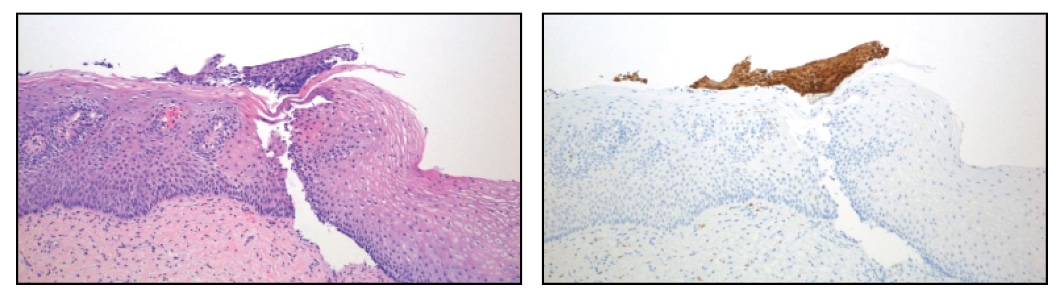
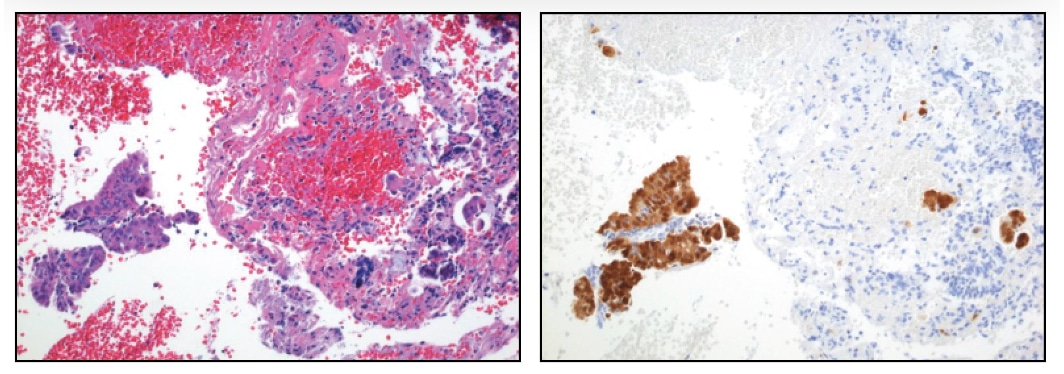
In problematic cases and in occult lesions, p16 also plays an important role. Dr. Wright shared an image of a biopsy that at least three pathologists who specialize in gynecologic pathology had called non-CIN in the ATHENA study. “When we do the p16 staining, though, what you can see is there’s a little area of p16 positivity. When you look at higher power at that area with p16 positivity, there’s a substantial amount of cellular atypia present. And this was a very small high-grade lesion which was missed by three pathologists.” He displayed two more cases in which small fragments of high-grade disease were initially missed, then detected once p16 staining was performed. (See “Detection of occult lesions.”)
The objectives of the CERTAIN study were to: 1) evaluate the performance of p16 immunohistochemistry as an adjunctive diagnostic aid to H&E-stained slides for the identification of high-grade disease (CIN 2+ status), and 2) assess the performance of published criteria for selecting which biopsies should be stained with p16.
It began with 1,100 H&E-stained cervical biopsies that were initially reviewed by Dr. Wright and Mark H. Stoler, MD, of the University of Virginia School of Medicine, using a three-tiered CIN terminology. If they agreed on a diagnosis, they had an expert H&E diagnosis. If they didn’t agree, it went to a third gynecologic pathologist who reviewed it. “And if two of the three diagnoses agreed, we ended up with our expert H&E diagnosis,” Dr. Wright said. “If all three of us disagreed, we reviewed the slides in conference and came up with a final diagnosis.”
After an H&E-based diagnosis was made, they completed the entire process a second time, but this time looking at both the H&E and the p16-stained slides for every case. They looked at the rate of positivity for p16 by whether the consensus diagnosis was normal, CIN 1, CIN 2, or CIN 3+, using H&E only, and then looking at both H&E and p16. For within normal limit diagnoses, 7.4 percent of the cases were p16 positive. “That decreased to 1.3 percent when we looked at the H&E together with the p16. Fifty-eight percent of the CIN 1 lesions were p16 positive made with H&E-only diagnosis and 50 percent if we had both H&E and p16. And in this study, approximately 100 percent of CIN 2 and CIN 3+ lesions were p16 positive.”
The biopsies were divided into four reading sets of 275 biopsies each, and each set was reviewed by 17 or 18 (of a group of 70) community surgical pathologists who routinely look at cervical biopsies. “And they did the same process the experts did,” Dr. Wright said. “They looked at the slides using the H&E-stained slides only, they had a one-month washout period, and then they re-diagnosed them using H&E together with p16.” There were more than 19,250 reads per method.
They compared the community pathologist H&E diagnoses versus the expert H&E diagnoses and the community H&E plus p16 diagnoses versus the expert H&E diagnoses. The study examined the following: accuracy, meaning overall percent agreement between the community pathologists and the expert pathologists; sensitivity, meaning their agreement on “positive” cases (CIN 2 or greater); and specificity, meaning their agreement on the “negative” cases.
When the community pathologists had p16 available to them, the sensitivity for high-grade disease went from 85.7 percent to 92 percent, while specificity went from 91.8 to 93 percent (not significant). Overall percent agreement (sensitivity and specificity combined) went from 89.9 percent to 92 percent—“a 2.1 percent increase, which is highly significant,” Dr. Wright pointed out. “So they had an improvement in the sensitivity and overall accuracy using p16 compared to when they only had H&E alone to make the diagnosis.”
In the study, the experts were no different than the community pathologists in their ability to benefit from having a p16-stained slide, Dr. Wright said. “What we see is that when we improve the ability of the experts to make the diagnosis, p16 actually works better for the community pathologists because now they’re comparing it versus the real gold standard, which is the expert’s H&E plus p16 diagnosis.”

Using as the gold standard the experts’ diagnosis made with both H&E and p16, the community pathologists’ sensitivity rose from 74.7 percent to 86.2 percent. “That’s an 11.5 percent increase in sensitivity,” Dr. Wright emphasized. “That doubles over what we saw using the expert H&E alone diagnosis. We’ve doubled the improvement in sensitivity because the gold standard is better. We’ve also doubled the improvement in specificity. It’s now 2.6 percent better, and this is significant.” Accuracy also doubles, he said, pointing to a 4.6 percent improvement. “So we see even a better effect of allowing the community pathologists to read with p16 when we have the good expert diagnosis, which is that made by H&E with p16.”
When looking at the performance of individual community pathologists, some were found to have showed improved sensitivity when they had p16 made available to them, but they had small reductions in specificity. A smaller group of pathologists showed an increase in specificity but a small reduction in sensitivity. “Importantly, not a single pathologist had reduced sensitivity and reduced specificity when they had p16 made available to them,” Dr. Wright said. “All of them got better in both sensitivity and specificity or either sensitivity or specificity.”
Further, “there was, as you would predict, an improvement in intraobserver agreement with the diagnosis of CIN 2+,” he said. “It went from moderate agreement with a kappa of 0.58 on H&E alone to substantial agreement, kappa of 0.76, when they had p16 available to review with the H&E slide.”
These results are in press (Stoler MH, et al. Am J Surg Pathol. 2018).
The aim of the second part of the CERTAIN study was to determine the efficacy of the LAST (Lower Anogenital Squamous Terminology) criteria for identifying which cases should have p16 IHC (Darragh TM, et al. Arch Pathol Lab Med. 2012;136:1266–1297).
“During read one, when the community pathologists only were looking at H&E-stained slides, we asked them whether or not they wanted a p16 according to the LAST criteria for reviewing this slide,” Dr. Wright said. “Before we asked them, we went through the LAST criteria with them, so they were aware of exactly what they were.” There was a wide variation in requests for p16 staining. Overall, they wanted p16 in 42.3 percent of the biopsies. By comparison, Dr. Stoler asked for adjunctive p16 IHC in 19 percent of cases, Dr. Wright in 30 percent of cases. “Not much different from the individual pathologist,” Dr. Wright noted.
The LAST criteria (situations in which p16 IHC is recommended) are as follows: To aid in the differential diagnosis between CIN 2+ and a mimic of precancer (immature squamous metaplasia, reparative epithelial changes, atrophy, or tangential cutting), anytime a morphologic diagnosis of CIN 2 is considered, as an adjudication tool for cases with professional disagreement if the differential diagnosis includes CIN 2+, and as an adjunct to morphologic assessment for biopsy specimens interpreted as ≤CIN 1 that are at high risk for missed high-grade disease. “These are women with a prior HSIL Pap test, ASC-H, ASC-US, and HPV16 positive, or women who have atypical glandular cells. If you don’t see high-grade disease in those biopsies, you need to do p16 immunostaining.”
For the LAST biopsies (that is, those for which p16 was requested based on the LAST recommendations), sensitivity increased 11.8 percent, specificity increased 9.7 percent, and overall accuracy increased by 10.1 percent. “However, when we take the cases in which they said, ‘No, I don’t need to order a p16 on this particular case, H&E is all I need to make the diagnosis,’ in those cases, the sensitivity when they had p16 available increased just as much as it did in the LAST cases,” Dr. Wright said. Sensitivity increased from 73.1 percent to 84.1 percent in the non-LAST cases (those for which p16 wasn’t requested based on LAST criteria).
However, specificity took a small hit, dropping from 99.2 percent to 98.5 percent. And diagnostic accuracy, because of this loss in specificity, increased only 0.5 percent. “So the take-home to me is: We don’t really know when we need p16,” Dr. Wright said. “Not that the LAST criteria are wrong; it’s just that in cases in which we think we don’t need a p16, adding p16 to the case will give you an improvement in your ability to detect high-grade disease.”
The conclusions, then, of the CERTAIN study: Adjunctive use of p16 with H&E-stained slides improved accuracy and sensitivity of community pathologists compared to both reference standards when p16 is used on every slide. “Positive effects doubled when using a more accurate reference standard,” Dr. Wright said. “That’s the experts who had p16 available, because everybody improves with p16.” P16 staining used in accordance with the LAST criteria improved accuracy, sensitivity, and specificity. “We saw an equally large improvement in sensitivity when performed on the non-LAST cases, but we saw a small loss in specificity of 0.8 percent.”
While agreement among all pathologists improves with the use of p16, it remains unclear which non-LAST cases need p16, Dr. Wright added. “None of us wants to do every single case with p16. It would be expensive. It is more work for the laboratories. But we haven’t yet come up with a good decision about how we can get improved sensitivity by adding other categories in the ones that LAST already lists.”
Recognizing the need to evaluate morphology based on H&E is important. “P16 doesn’t totally surmount, or doesn’t totally replace, the H&E,” he said. “You clearly do not want to upgrade a morphologic CIN 1 that is p16 positive, and in fact something that is clearly a morphologic CIN 1 probably doesn’t need to be stained or shouldn’t be stained with p16. And finally, you need to interpret the p16 stain. Don’t overcall patchy areas as being p16 positive. They’re negative.”
[hr]
Anne Ford is a writer in Evanston, Ill.
The full webinar is available at www.captodayonline.com.