 CAP TODAY Pathology/Laboratory Medicine/Laboratory Management
CAP TODAY Pathology/Laboratory Medicine/Laboratory Management
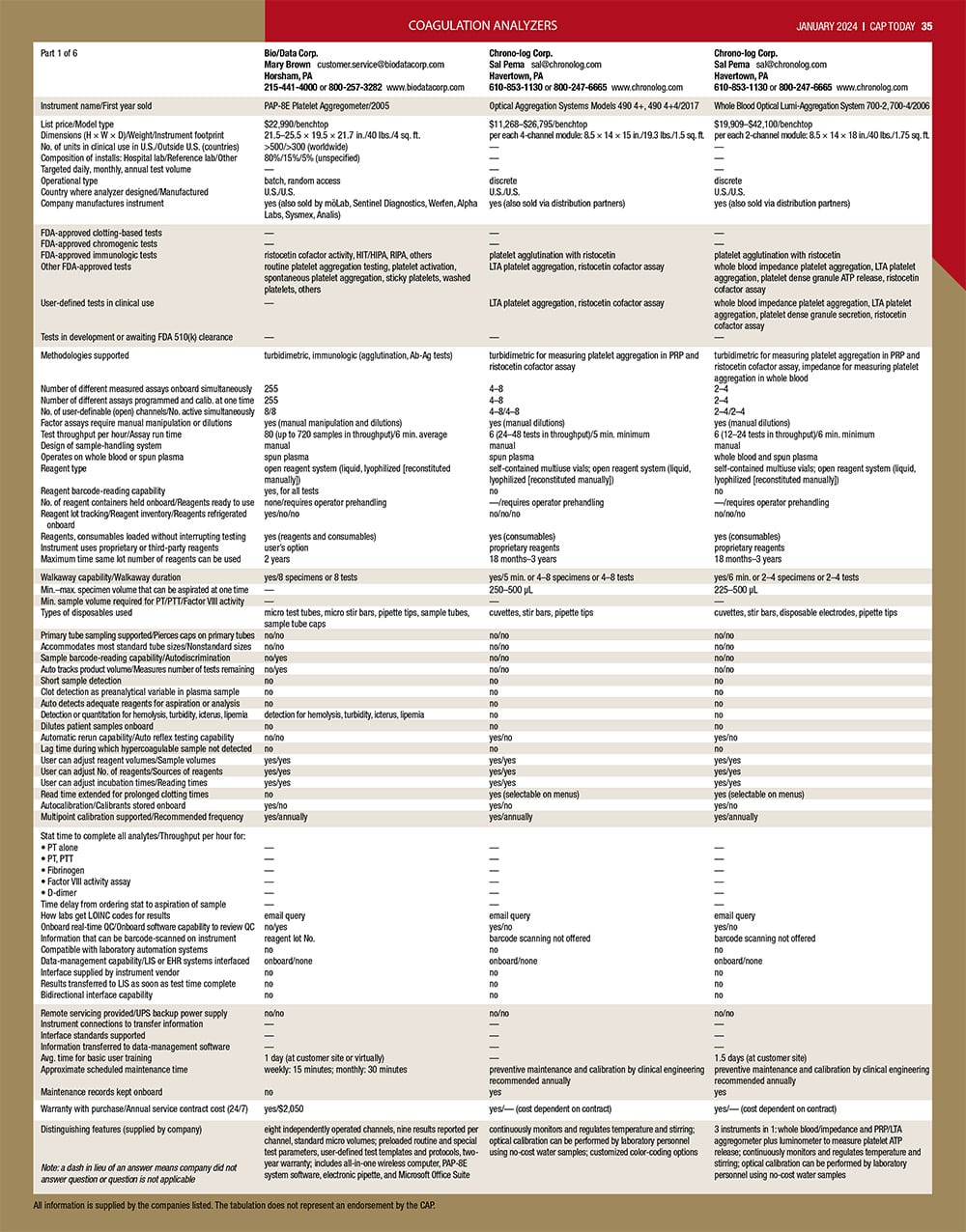
Company:
Contact:
Email:
City, State:
Phone:
Website:
Instrument name/First year sold:
List price/Model type:
Dimensions (H × W × D)/Weight/Instrument footprint:
No. of units in clinical use in U.S./Outside U.S. (countries):
Composition of installs: Hospital lab/Reference lab/Other:
Targeted daily, monthly, annual test volume:
Operational type:
Country where analyzer designed/Manufactured:
Company manufactures instrument:
FDA-approved clotting-based tests:
FDA-approved chromogenic tests:
FDA-approved immunologic tests:
Other FDA-approved tests:
User-defined tests in clinical use:
Tests in development or awaiting FDA 510(k) clearance:
Methodologies supported:
Number of different measured assays onboard simultaneously:
Number of different assays programmed and calib. at one time:
No. of user-definable (open) channels/No. active simultaneously:
Factor assays require manual manipulation or dilutions:
Test throughput per hour/Assay run time:
Design of sample-handling system:
Operates on whole blood or spun plasma:
Reagent type:
Reagent barcode-reading capability:
No. of reagent containers held onboard/Reagents ready to use:
Reagent lot tracking/Reagent inventory/Reagents refrigerated onboard:
Reagents, consumables loaded without interrupting testing:
Instrument uses proprietary or third-party reagents:
Maximum time same lot number of reagents can be used:
Walkaway capability/Walkaway duration:
Min.–max. specimen volume that can be aspirated at one time:
Min. sample volume required for PT/PTT/Factor VIII activity:
Types of disposables used:
Primary tube sampling supported/Pierces caps on primary tubes:
Accommodates most standard tube sizes/Nonstandard sizes:
Sample barcode-reading capability/Autodiscrimination:
Auto tracks product volume/Measures number of tests remaining:
Short sample detection:
Clot detection as preanalytical variable in plasma sample:
Auto detects adequate reagents for aspiration or analysis:
Detection or quantitation for hemolysis, turbidity, icterus, lipemia :
Dilutes patient samples onboard:
Automatic rerun capability/Auto reflex testing capability:
Lag time during which hypercoagulable sample not detected:
User can adjust reagent volumes/Sample volumes:
User can adjust No. of reagents/Sources of reagents:
User can adjust incubation times/Reading times:
Read time extended for prolonged clotting times:
Autocalibration/Calibrants stored onboard:
Multipoint calibration supported/Recommended frequency:
Stat time to complete all analytes/Throughput per hour for::
• PT alone:
• PT, PTT:
• Fibrinogen:
• Factor VIII activity assay:
• D-dimer:
Time delay from ordering stat to aspiration of sample:
How labs get LOINC codes for results:
Onboard real-time QC/Onboard software capability to review QC:
Information that can be barcode-scanned on instrument:
Compatible with laboratory automation systems:
Data-management capability/LIS or EHR systems interfaced:
Interface supplied by instrument vendor:
Results transferred to LIS as soon as test time complete:
Bidirectional interface capability:
Remote servicing provided/UPS backup power supply:
Instrument connections to transfer information:
Interface standards supported:
Information transferred to data-management software:
Avg. time for basic user training:
Approximate scheduled maintenance time:
Maintenance records kept onboard:
Warranty withWarranty with purchase/Annual service contract cost (24/7) purchase/Annual service contract:
Distinguishing features (supplied by company):
Note: a dash in lieu of an answer means company did not answer question or question is not applicable:
Panelists on viscoelastic and other coag assays
January 2024—Viscoelastic assays and other coagulation tests were front and center when CAP TODAY publisher Bob McGonnagle on Nov. 20 convened seven people in an online roundtable. Oksana Volod, MD, and Eric Salazar, MD, PhD, and five company representatives weighed in on, among other things, appropriate test use, automation, and laboratory-developed tests. What they said begins here; CAP TODAY’s guide to coagulation analyzers begins here.

Dr. Volod
Oksana Volod, you have now written the first book on viscoelastic testing that’s designed to speak directly to pathologists and others in clinical laboratories. Where are we with the adoption of viscoelastic testing? Will it become more mainstream now in the repertoire of the people who do thrombosis and hemostasis testing?
Oksana Volod, MD, director of coagulation consultative service and professor of pathology, Cedars-Sinai Medical Center; associate professor of pathology, David Geffen School of Medicine at UCLA: TEG [thromboelastography], the first viscoelastic assay, was developed before partial thromboplastin time and was initially used in liver transplant and cardiac surgeries. In 2000, when we had a cell-based model of hemostasis, there was an understanding that there was a role for platelets, red blood cells, and other cells or elements to form a clot, and that plasma-based assays, like PTT and PT, will not provide comprehensive information. That’s when interest in viscoelastic testing emerged and when it was adopted, mainly by anesthesiologists, perfusionists, people who were in the OR. Laboratories were not that receptive because there were validation steps they would have to be involved in, and there was a disconnect at some point between laboratorians and anesthesiologists and surgeons. They wanted to bring viscoelastic assays in-house, but laboratories were resistant and questioned where the device would be located—in the laboratory or at the point of care. However, the laboratory was instrumental in validation and in maintaining the competency of their personnel. The whole process was a collaboration.