
[wpdatatable id=30]
[one_third]
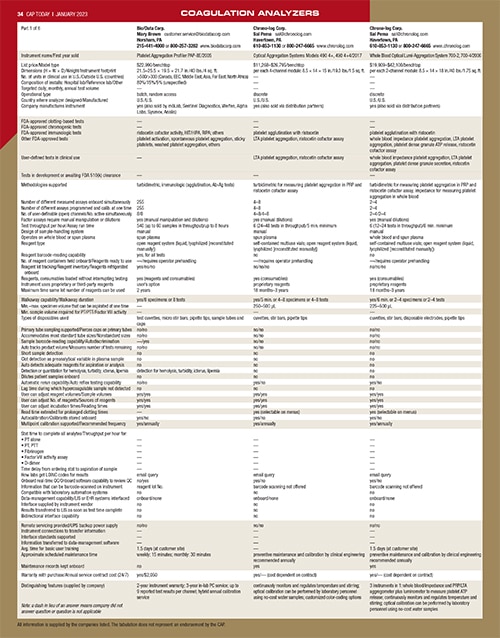
Download Excel version
[/one_third]
[two_third_last]
Volume? Space? Automation decisions in coagulation
January 2023—Automation and point-of-care, reflex, and viscoelastic testing were some of what came up when a group spoke with CAP TODAY publisher Bob McGonnagle in late November about hemostasis testing. Also tossed in: Results reporting to the EHR, which “can always be improved,” said Eric Salazar, MD, PhD, of University of Texas Health San Antonio. And D-dimer, one of the pandemic’s “health care heroes,” said Nichole Howard of Diagnostica Stago.
Here’s what they said about all that and more.
Dr. Russell Higgins, what is top of mind as you look at the field of hemostasis now? I put this in two parts—the routine, high-volume, largely heavily instrumented side and then the specialty assay areas.
Russell Higgins, MD, professor, clinical, University of Texas Health San Antonio, and medical director, University Health System Pathology Services: If we’re talking about instrumentation, it’s automation—track systems, integration into larger track systems, and the automation that goes in the box of coagulation analyzers, like HIL [hemolysis, icterus, lipemia] modules. Those are changing. Coagulation is late to the game in terms of incorporating HIL into the workflow compared with chemistry, which has been doing this for some time.
Dr. Eric Salazar, I’m going to ask you the same question. I know you have a specialty in the more esoteric components of the coagulation cascade.
Eric Salazar, MD, PhD, associate professor, clinical, University of Texas Health San Antonio, and member, CAP Hemostasis and Thrombosis Committee: My top three answers are automation, automation, and automation. In addition to what Dr. Higgins said, we’re talking about ease of use. The pandemic taught us that we’re going to have shortages of workers—we currently have shortages of medical laboratory scientists—and supplies. There were crunches during the pandemic such that the easier the device was to use, the more sustainable the whole process. And that’s why we think about automation not only for routine tests but also for some of the more esoteric tests that require manual processes. Can we get these tests automated in the event you need an esoteric test more rapidly? The more automated it is, the better it is for us so we don’t need specialized medical laboratory scientists.
As Dr. Higgins and I explored—we recently wrote a chapter on automation and coagulation—when we talk about automation we’re talking not only about connecting the track systems or the inside of the box, but also about middleware and what the software can do to make running the tests easier.
Matt Modleski, what’s top of mind as you look to coagulation testing and the laboratory and in the networks and systems you work with?
Matt Modleski, executive vice president of corporate/business development, Orchard Software: As these tests become better at the point of care, we see a lot of testing moving closer to the patient. Our two jobs as a software company are, one, be ready when a new test comes to market so we can integrate it smoothly into the lab. We need a little advanced warning if there are new analyzers coming so we can work on interfaces and the things that make bringing the new test and new analyzer to market easy.
The other is the location of testing, point-of-care tests. That trend will continue because it makes sense from the perspective of the cost of other health care. The closer we can get a test result to the patient, when the clinician wants it, the better the chance of that patient getting the care they need in a timely fashion and staving off downstream costs. When we think about coagulation, we’re looking at the same four things we look at with almost all testing, which is: Is it going to move to point of care or is it already there, and how efficient is it? If there’s new technology coming, are we ready for it? And as those trends move, where is the biggest bang for the buck from a reimbursement or a patient treatment perspective? Are we ready to help that area of testing and treatment?
Continue reading …
[/two_third_last]