
Amy Carpenter Aquino
July 2023—Though it’s been suggested that newer drugs have made cytomegalovirus less relevant in patients with inflammatory bowel disease, CMV remains an important opportunistic infection in patients with IBD. Knowing where to biopsy and how many are needed is one of the histologic challenges, said Joseph Misdraji, MD, associate professor of pathology, Yale School of Medicine, in a CAP22 session.
Another is defining high-grade disease. Patients with high-grade disease may be more likely to benefit from antiviral therapy, according to several studies, he said, but there is no standard definition.
CMV is a double-stranded DNA virus in the herpes family that infects 66 to 75 percent of people in Western populations. Primary infection is usually asymptomatic or can resemble Epstein-Barr virus before entering a latent phase.
“What we’re often looking at is CMV reactivation,” Dr. Misdraji said, “either in the population or even in patients with inflammatory bowel disease, where the CMV replication begins in the target organ, such as the colon, and then becomes disseminated after some time into peripheral blood.”
Primary CMV infection in immunosuppressed patients with IBD is a severe illness associated with viremia, tissue damage, pneumonia, and hemophagocytic lymphohistiocytosis. It can be fatal even if treated with ganciclovir, said Dr. Misdraji, who is also director of histology in the Department of Pathology at Yale and associate pathologist at Yale New Haven Hospital. More often seen in pathology practice, he said, is reactivation of CMV promoted by the upregulation of inflammatory mediators in patients with IBD. “This often results in nonresponse to their IBD therapy.”
CMV reactivation occurs more often in patients with ulcerative colitis (38 percent) than in patients with Crohn’s disease (11 percent), Dr. Misdraji said, noting, “The cytokine milieu of ulcerative colitis favors CMV reactivation.” CMV reactivation depends on tumor necrosis factor-α, and in ulcerative colitis TNF-α favors CMV reactivation. In Crohn’s disease, interferon-γ exhibits antiviral properties.
There has long been controversy in the literature, he said, about whether CMV reactivation is a marker of severe inflammatory disease that has no bearing on prognosis or whether it is pathogenic and exacerbates the colitis, with worse outcome. Most studies at this point, though not all, support that CMV in patients with IBD is associated with increased patient mortality, nonresponse to immunosuppressive therapy, higher rates of colectomy, longer hospital stays, and higher costs, and that treating CMV restores steroid responsiveness, reduces the colectomy rate, and improves the outcome, he said.
CMV can exacerbate colitis by promoting proinflammatory cytokine production; replicating in the endothelial cells, resulting in microthrombi and tissue ischemia; and disrupting epithelial tight junctions in the gut, enhancing bacterial translocation.
“Some people have suggested that CMV may not be as relevant today in the age of biologics as it was years ago when everyone was on steroids and thiopurines,” Dr. Misdraji said. Those drugs and cyclosporines do raise the risk for CMV, whereas the newer anti-TNF agents, such as infliximab and adalimumab, are not associated with an increased risk of CMV reactivation.

“It turns out that the new kid on the block is vedolizumab,” he said, “and that does increase the risk of severe CMV,” by targeting the α4β7 integrin that homes lymphocytes to the gut. “Ultimately, many of these therapies are given sequentially or concurrently, and CMV today remains an important opportunistic infection in this patient population.”
For clinicians, diagnosing CMV disease versus infection in patients with IBD is a challenge, Dr. Misdraji said. “Many of these patients have CMV infection, meaning they’ve already been carrying it and they’re infected with the virus,” he said, “but how do we demonstrate there’s active CMV disease?” Endoscopy is one modality, and some but not all studies have found clinically relevant CMV disease to be associated with deep ulcers. “Serology has very limited utility in reactivation,” he noted. IgM occurs in primary CMV infection, and most patients have an IgG.
CMV antigenemia assays detect pp65 antigen in circulating lymphocytes, he said, and are not entirely predictive of CMV activity in the colon.
CMV PCR in blood leukocytes is a relatively rapid test and thus used frequently, “almost as a screening test,” he said. But since CMV involves the blood only after days or weeks of viral replication in the colon, a positive result is helpful but a negative result may be less so. There will be a positive value in 48 percent of patients with an IHC diagnosis and 60 percent if there are numerous inclusions. A high viral level result supports treatment, but cutoffs have not been established.
PCR in colonic tissue is one of the two gold standards. “High values of quantitative PCR in the colon do correlate with active disease, and the test is usually negative in biopsies that do not have inclusions,” Dr. Misdraji said. The other is histology with immunohistochemistry, which “is a gold standard across numerous white papers. Ultimately, we are the gold standard,” he said.
Where to biopsy and how many biopsies are needed is the question. “Not every biopsy fragment has inclusions, and not every biopsy from every site has inclusions. Ulcers and granulation tissue have the highest likelihood of having inclusions, so biopsies from ulcerated areas are going to be more productive,” he said. Some studies have shown that up to 16 biopsies may be necessary to demonstrate CMV in a patient who has CMV disease, but it’s possible to reduce that number by focusing on ulcerated areas (McCurdy JD, et al. Inflamm Bowel Dis. 2015;21[12]:2833–2838; Roblin X, et al. Am J Gastroenterol. 2011;106[11]:2001–2008).
McCurdy, et al., found in their retrospective study of 68 patients that biopsy location and number are important when assessing for CMV. In the majority of patients with ulcerative colitis, CMV was detected from the left colon. Among patients with Crohn’s disease, a substantial number had CMV detected from only the right colon.
Some studies have cast doubt on whether IHC is necessary to diagnose viral infections in humans, including CMV in patients with IBD, Dr. Misdraji said. H&E is highly specific (92 to 100 percent) but has variable sensitivity (10 to 87 percent). “We’ve all had that situation where we get a CMV stain and it’s positive,” but the inclusions were not seen on the initial H&E.
IHC improves sensitivity to 78 to 93 percent, he said, though some question its necessity because clinically relevant infections generally have inclusions on H&E (Solomon IH, et al. Am J Clin Pathol. 2017;147[1]:96–104). “But there are always cases in which we just didn’t see them, or they’re atypical inclusions, they’re a little smaller than usual, and you’re surprised by the stain.” The European Crohn’s and Colitis Organization guidelines recommend tissue PCR or IHC for diagnosing CMV in the setting of immunomodulator-refractory IBD.
The question is which patients need to be treated. Here there is growing evidence that CMV disease can be stratified into low- and high-grade disease, Dr. Misdraji said, and that high-grade disease is associated with a higher colectomy rate but may also be more likely to benefit from antiviral therapy. “The big issue for us at this point is that all the studies are using different definitions of what constitutes high-grade disease for us to report,” he said.
Kuwabara, et al., used resection specimens and defined high-grade disease as greater than 10 inclusions in any one histologic section. That was the first study that found an association between high-grade disease and a worse outcome, shorter interval to colectomy, and steroid resistance, Dr. Misdraji said (Kuwabara A, et al. J Gastroenterol. 2007;42[10]:823–829).
A 2011 article on CMV reactivation in ulcerative colitis patients defined high-grade disease as visible inclusions on H&E versus only on the IHC stain (Nguyen M, et al. Ulcers. 2011;2011:282507). A study published in 2015 reported that the beneficial effect of treatment was most notable in patients with high-grade disease, defined as more than five viral inclusions in any one biopsy fragment. “The number 5 was chosen arbitrarily,” the authors wrote, “as a cut-off point based on a subjective assessment of what constituted a heavy viral load” (Jones A, et al. Clin Gastroenterol Hepatol. 2015;13[5]:949–955).
“Once that study showed association, other people looked at the same number,” Dr. Misdraji said, among them Zagórawicz, et al., who found that five or more CMV IHC-positive cells per biopsy section were indicative of a greater colectomy risk, though response to ganciclovir was not clearly better in that group (Zagórowicz E, et al. J Crohns Colitis. 2016;10[10]:1205–1211).
Clos-Parals, et al., in their study of 46 cases, defined high-grade disease as greater than two inclusions by IHC on a single tissue fragment because at five inclusions they found no association with a higher colectomy rate, Dr. Misdraji said (Clos-Parals A, et al. J Crohns Colitis. 2019;13[3]:385–388). Oh, et al., used five inclusions and reported finding no difference in outcome between high- and low-grade CMV disease (Oh SJ, et al. Scand J Gastroenterol. 2019;54[8]:976–983).
“Looking at the outcome or response to antiviral therapy, the majority of studies show that high-grade disease matters,” he said, “but not all do.” Treatment may be more appropriate for patients with moderate to severe steroid-refractory relapses with a high viral load, he said, “whereas a negative blood CMV PCR test result, a very low quantitative PCR in the tissue, and maybe a single inclusion on IHC can support a decision to abstain from antiviral therapy because there are risks to ganciclovir.”
Ganciclovir is generally given with immunosuppressive therapy, Dr. Misdraji said, “because you want the synergistic effect of reducing the viral replication but also keeping down the inflammation,” especially when anti-TNF-α is used. If CMV disease becomes severe and systemic, immunosuppressive therapy is discontinued.
Dr. Misdraji summed up with the following suggestions for the histologic assessment for CMV:
- Look for CMV inclusions on the H&E stain of severely inflamed or ulcerated biopsies and confirm with IHC. “We’ve all seen ulcers that have funny fibroblasts, and then when you get the stain they’re negative.”
- Order CMV IHC in severely inflamed or ulcerated biopsies, particularly but not exclusively if you are aware that the patient is refractory to their steroid therapy, or if clinically requested.
- Report whether the viral inclusions are visible on the H&E or only on the IHC. “Even if the IHC is positive, I’ll go back to the H&E and report if I can see them on the H&E because that may indicate more severe disease,” he said. “And I will report the number of IHC-positive cells in the single most involved tissue fragment, knowing that a threshold for high-grade disease is not established. I’ll at least give a number or say whether they’re numerous or it’s a single inclusion.”
- Don’t overinterpret lymphocytes or plasma cells that are staining as relevant.
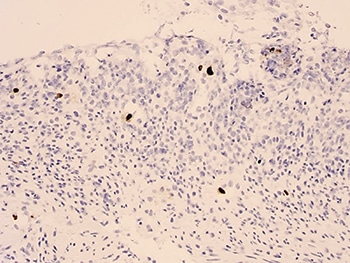
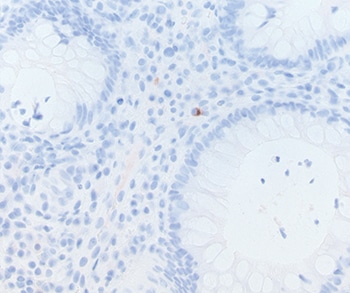
In Fig. 1 is an example of an IHC stain showing numerous inclusions. “They should be large cells with nuclear expression,” Dr. Misdraji said. In Fig. 2 is a plasma cell that shows some cytoplasmic staining. “Most people do carry CMV,” he said, but cytoplasmic staining of small lymphocytes or plasma cells, as in Fig. 2, is not indicative of active CMV disease.
Amy Carpenter Aquino is CAP TODAY senior editor.