 CAP TODAY Pathology/Laboratory Medicine/Laboratory Management
CAP TODAY Pathology/Laboratory Medicine/Laboratory Management

Says Dr. Theel, “We showed improved sensitivity early on, no change in sensitivity at later stages, and equivocal specificity relative to the standard algorithm.” The sensitivity of the modified algorithm in patients with acute disease (73 to 77 percent, according to the literature, compared with 35 to 50 percent by the standard algorithm) is its primary advantage, she says (Fig. 1), though its sensitivity remains imperfect. “Early on in disease a negative result still does not rule out infection.” Another advantage of the modified algorithm: Antibodies to a wider range of Borrelia species can be detected. “The blots we use in North America are specific for B. burgdorferi strain B31,” she says. “They will not effectively detect antibodies to other species of Borrelia.”

Figure courtesy of Elitza Theel, PhD, D(ABMM).
Sfeir MM, et al. J Clin Microbiol. 2022;60[5]:e02528-21; Branda JA, et al. Clin Infect Dis. 2011;53[6]:541–547; Pegalajar-Jurado A, et al. J Clin Microbiol. 2018;56[8]:e01943-17; Molins CR, et al. J Clin Microbiol. 2016;54[11]:2726–2734.
Suppose a patient had Lyme disease previously and presents a year later with similar symptoms, she says. “Initially they have six bands, but then you retest them and they’ve moved up to 10 bands over a two-week period. That would be highly suggestive that this is a new recent reinfection.” With the two-step EIA sequence, “if you test them now they’re going to be positive because of that prior infection, and if you test them in two weeks they’re still going to be positive. You aren’t able to tell if there is a progression or expansion of the immune response.” The index values from the ELISA readouts can provide information about whether the result is a “high-positive,” which would be a high number, or a “low-positive,” which would be a value near the threshold. “But it’s not a true quantitative assay, so clinicians shouldn’t be using this to monitor values or levels over time. Plus, we do not report index values on our patient results.”
At Mayo Clinic, the first-tier test is a VIsE/pepC10/OspC total antibody EIA. “If those are reactive, we automatically reflex to two separate EIAs looking for IgM and IgG antibodies to whole-cell sonicate material from Borrelia burgdorferi,” she says. If either of the supplemental assays is positive, the patient is considered positive.
Another option for the second-tier test is a single whole-cell sonicate IgM/IgG ELISA, which does not differentiate between the classes of antibody present. “It’s potentially beneficial from a laboratory perspective because you’re only running a single EIA, but it doesn’t give enough information from a clinical interpretation perspective,” Dr. Theel says.
Guidance from the CDC and others says IgM-specific results for Lyme should not be interpreted in patients with more than 30 days of symptoms. “That’s because that IgM might be there due to a past infection or it may be present due to cross-reactivity leading to a false-positive.” With the single IgG/IgM ELISA, “you can’t tell if it’s reactive or positive because you’re detecting IgM, in which case you’d want to know if the patient has more or less than 30 days of symptoms, or if you’re detecting just IgG.”
Another option for the lab would be to provide two different orders: a first-tier test that automatically reflexes to two separate IgG and IgM EIAs, to be ordered only for patients with fewer than 30 days of symptoms, and a first-tier test that automatically reflexes to a single IgG EIA, to be ordered only for patients with more than 30 days of symptoms. “But that would likely be challenging for clinicians, so we offer a single orderable with a reflex to IgM and IgG and include in comments that the IgM should not be considered for patient management if he or she has more than 30 days of symptoms.”
Result reporting for the modified algorithm at Mayo Clinic is sequential rather than simultaneous, with the laboratory reporting a positive first-tier test, owing to a limitation of the laboratory information system. “My preference would be that the results would be reported after all testing is completed, with the final interpretive comment, because when you report a positive result for the first-tier test—which is what the package inserts and guidance documents recommend—there are still providers who are confused and think that this is the final result, and that may lead to additional or potentially unnecessary treatment.”
At Mayo Clinic, when the initial test is positive, the lab says in the comment that it is not diagnostic and that supplemental testing has been ordered by reflex. “But that of course depends on the clinician reading the comment, which does not always occur,” she says.
The Association of Public Health Laboratories released a Lyme disease algorithm reporting aid, to which Dr. Theel contributed and which she recommends laboratories refer to when putting together their Lyme testing algorithm. In Fig. 2 is Table 4 from the document (the full document is at https://shorturl.at/jqt01).
Neuroinvasive Lyme disease, which occurs in up to 15 percent of untreated Lyme disease patients, requires a different testing strategy. “We should not be using the modified or standard two-tiered testing algorithms on spinal fluid,” which were validated strictly on serum, Dr. Theel says. The recommendation for neuroinvasive Lyme, alongside clinical presentation, is to perform a Lyme antibody index test. “You compare the level of Lyme antibodies in cerebrospinal fluid versus serum relative to total immunoglobulin in those two sample types. It’s a much more specialized testing process to ensure that any antibodies detected in spinal fluid are there due to intrathecal synthesis versus passive diffusion of the antibodies from serum into the spinal fluid.” Mayo Clinic implemented the assay in 2018.
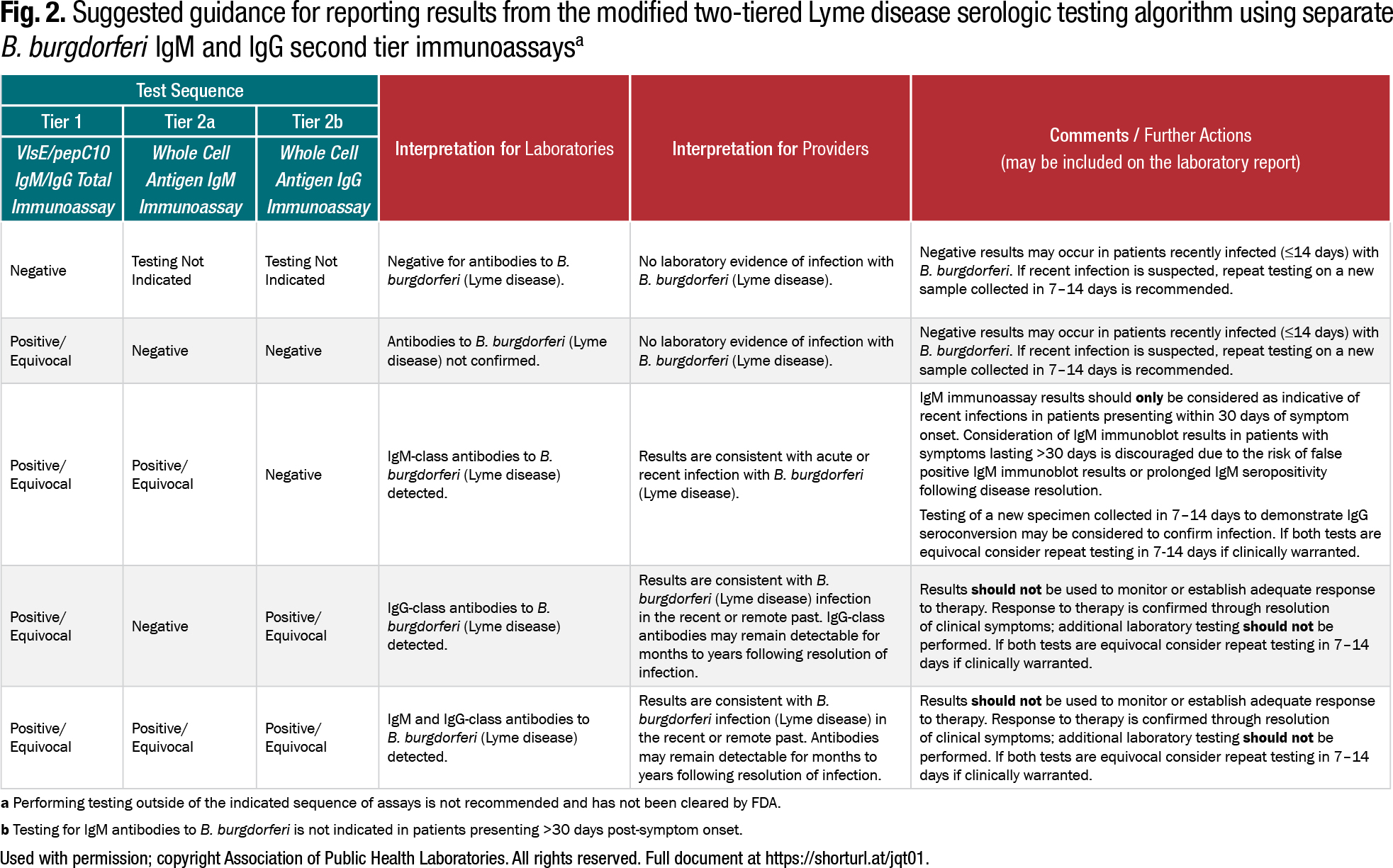 Used with permission; copyright Association of Public Health Laboratories. All rights reserved. Full document at https://shorturl.at/jqt01.
Used with permission; copyright Association of Public Health Laboratories. All rights reserved. Full document at https://shorturl.at/jqt01.
Neuroinvasive Lyme disease has both peripheral and central nervous system manifestations: cranial neuritis, radiculoneuritis, and plexopathies, or meningitis, encephalitis, and myelitis. “And typically you see a lymphocytic predominance in spinal fluid testing,” she says. Per the Infectious Diseases Society of America, a patient with one or more of these symptoms and an epidemiologically plausible exposure to ticks infected with B. burgdorferi would meet the criteria for testing.
The CDC doesn’t differentiate between systemic and neuroinvasive Lyme disease, Dr. Theel says. “Whether you have neuroinvasive Lyme or just Lyme, you’re counted as a Lyme disease case. So we don’t have a good sense of the prevalence of neuroinvasive Lyme disease in the U.S.” Mayo Clinic sees a peak of neuroinvasive Lyme every summer and fall, at about five percent during August and September annually. “So I think it’s much more prevalent than we think.”
Neuroinvasive Lyme is often thought of in connection with B. garinii, she says, a Borrelia species found in Europe. “So we think that’s a European manifestation of Lyme disease. But it’s also a manifestation of infection with Borrelia burgdorferi, and I don’t think we’re as cognizant of that fact or consider it as frequently as we perhaps should.”
Charna Albert is CAP TODAY associate contributing editor.