 CAP TODAY Pathology/Laboratory Medicine/Laboratory Management
CAP TODAY Pathology/Laboratory Medicine/Laboratory Management

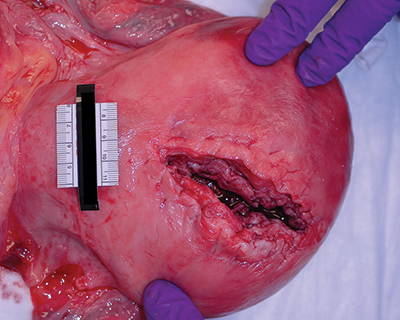
Fig. 2. Uterine rupture. A woman with an intrauterine pregnancy of estimated gestational age 32 weeks was found unresponsive at home. Resuscitation efforts were made. At the hospital, a caesarian section procedure was begun, and approximately 1500 mL of blood were evacuated from the peritoneal cavity. The viable baby was delivered and the uterus sutured, but the mother did not regain signs of life despite fluid and blood product provision and continued advanced life-support measures.
Obstetric hemorrhage was the leading cause of maternal mortality in the United States for the years 1998 to 2005 by a small margin. In addition, the majority of deaths from hemorrhage are considered preventable upon review. The number of women experiencing hemorrhage increased during the interval, and, in 2006, 2.9% of births were complicated by maternal hemorrhage, with the increase found to be secondary to increased incidence of uterine atony. Death from hypovolemic shock can occur if hemorrhage is not adequately identified or controlled in the peripartum period. A ruptured splenic artery aneurysm, spontaneous hepatic rupture, postpartum uterine atony, abruptio placentae, placenta previa, ruptured ectopic pregnancy, uterine rupture (Fig. 2), postpartum uterine inversion, or any disruption in the tenuously balanced coagulation cascade can lead to catastrophic blood loss. Uterine atony has been cited as the most common cause (79%; N=25,654 women with postpartum hemorrhage), and numerous independent risk factors are identified, including age (<20 years or 40 or more years), caesarian section with labor, hypertensive diseases of pregnancy, chorioamnionitis, polyhydramnios, multiple gestation, antepartum hemorrhage, and retained placenta. In addition, multiple etiologies lead to the common pathway of DIC and consequent hemorrhagic shock. These include sepsis, retained dead fetus, retained placental material (Fig. 3), amniotic fluid embolism, intravascular hemolysis, pregnancy-induced hypertension, placental abruption/disruption, and trauma. Any suture lines, vaginal or cervical lacerations, and the uterus itself should be examined in an attempt to locate the source of the hemorrhage. If bleeding was clinically oozing or diffuse, thrombotic microangiopathies of pregnancy should be suspected. In these cases, a specific site of bleeding may not be elicited upon examination. Such cases include thrombotic thrombocytopenic purpura/hemolytic-uremic syndromes (TTP/HUS), HELLP syndrome (hemolysis, elevated liver enzymes, low platelet count), pregnancy-induced hypertension, acute fatty liver of pregnancy, antiphospholipid antibody syndromes, systemic lupus erythematosus/lupus vasculitis, or DIC. Fibrin thrombi, characteristic of DIC, can be identified or confirmed with a Weigert stain, which stains fibrin pink. Renal glomerular capillary loops are a common place to find these thrombi. Untreated, the mortality is high. In addition, a multitude of hereditary coagulopathies—including activated protein C resistance, factor V gene mutations, prothrombin 20210 G→A mutation, and hyperhomocysteinemia—may contribute to a poor outcome resulting from thrombotic events after peripartum hemorrhage. The likelihood of thromboembolism may also increase. Uncontrolled hemorrhage may result from complications of von Willebrand disease and, to a lesser extent, inherited or acquired hemophilias

Fig. 3. Retained placental material. Decidualized endometrium surrounds placental villi, consistent with retained placental materials. (10×, hematoxylin-eosin stained.)
TTP should be considered in the maternal patient suffering from a coagulation disorder. If possible, a premortem peripheral blood smear should be examined and the clinical workup reviewed. If the diagnosis was considered clinically—microangiopathic hemolytic anemia, altered mental status, renal failure, thrombocytopenia, fever—a hemapheresis or hematology consultation note might be available for postmortem review. Platelet thrombi may be more easily visualized if an immunostain for factor VIII is employed because this factor binds to the platelet surface. In the renal glomerulus, the lesions are more likely to be at the vascular pole. A factor VIII immunostain will also highlight the endothelial surface.
Hepatic diseases specific to the pregnant patient include acute fatty liver of pregnancy (AFLP), the HELLP syndrome, spontaneous hepatic rupture, hyperemesis gravidarum, and intrahepatic cholestasis of pregnancy. Although hyperemesis gravidarum and intrahepatic cholestasis rarely result in mortality, AFLP and HELLP may lead to maternal death.
AFLP often occurs with pregnancy-induced hypertension, although its incidence is only approximately 1 in 10,000 to 20,000 pregnancies. Still, there is up to 45% fetal death and up to 10% maternal death when the disease does manifest. Histopathologic findings include microvesicular steatosis and, later, cholestatic lobular hepatitis. If AFLP is suspected, histologic evidence may include a frozen section of liver stained with oil red O or a similar lipophilic compound because the fat is removed during routine specimen processing and will only be evident by clear round spaces in the tissue. Extramedullary hematopoiesis and megamitochondria may also be present. In HELLP syndrome, fibrin deposition and intrahepatic periportal hemorrhage are seen. Both AFLP and HELLP syndrome can lead to multiple complications, although the maternal mortality rate is significantly higher in AFLP. The mortality rate has been affected by improvements in supportive care measures and for AFLP is reported as 7% to 18% and for HELLP as 1% to 25%. Up to 70% of women with AFLP and only approximately 15% of women with HELLP will suffer from DIC and acute renal failure. It is interesting to note that women with AFLP or HELLP during pregnancy are more likely to have fetuses with a mitochondrial fatty acid beta-oxidation defect due to deficiency of LCHAD (long-chain 3-hydroxyacyl-coenzyme A dehydrogenase). Thus, if the infant survives, it is important to convey this diagnosis to the pediatric care team in order to provide proper care while testing for inborn errors of metabolism is underway. On the other hand, it was observed that maternal liver disease was 18.1-fold higher when the fetus was affected by a fatty acid oxidation defect. Spontaneous hepatic rupture is rare, with an incidence of approximately 1 in 100,000 pregnancies. The etiology is unclear but may be due to infarction from fibrin deposition in combination with hypovolemia. Minor external trauma, possibly even uterine contractions, may play a role. Hepatic rupture may also occur as a complication of other hepatic diseases during pregnancy, such as HELLP and AFLP. Maternal mortality from hepatic rupture approaches 50%.