
Editor: Frederick L. Kiechle, MD, PhD
Submit your pathology-related question for reply by appropriate medical consultants. CAP TODAY will make every effort to answer all relevant questions. However, those questions that are not of general interest may not receive a reply. For your question to be considered, you must include your name and address; this information will be omitted if your question is published in CAP TODAY.
[button color=”blue” size=”small” link=”https://captodayonline.com/q-a-submission/” target=”blank” ]Submit a Question[/button]
Q. When reviewing a smear, we observed scattered (rare) immature granulocytes during a scan. But when the 100-cell differential was performed, the immature granulocytes were not reflected. How do you report the presence of the immature granulocytes?
A. December 2019—The immature granulocyte (IG) fraction—metamyelocytes, myelocytes, and promyelocytes—can be quantified on modern peripheral blood analyzers as part of the six-part automated differential of the white blood cell count. The total number of cells counted for differentials is, of course, much higher by automated methods (30,000 cells on Sysmex platforms, for example) compared with a manual method (standardly 100 cells).
Therefore, as noted in the question, a low proportion of IGs detected by automated differential may not be reflected in a random 100-cell manual differential. This discrepancy may occur not only because of significant differences in the total cell count but also because of other factors affecting the peripheral blood smear. For example, immature cells, because of their relatively large size, tend to concentrate at the feathered edge, so their distribution may be less random across a slide than in a fluid state.
One strategy used by our hospital-based laboratory to address rare IGs is to add a white blood cell morphology comment to the manual differential of “slight left shift.” This signals that immature granulocytes are present but that they represent less than one percent of WBCs—that is, less than one cell per 100 on a standard manual differential. A parenthetical or footnoted statement with this additional information could also be included.
A related strategy is to avoid manual review for low IG fractions alone when using analyzers that produce an IG count. (With analyzers that only generate a flag that IGs are present, manual review is always recommended.) Recent studies highlight the accuracy of modern analyzers in identifying IGs and advocate for reflex release of these automated values without a flag for manual review at low IG fractions (less than three percent to less than 10 percent, as suggested by varying sources). Automated IG fractions may be overestimated due to a systematic positive error, and flag for manual review is appropriate at high proportions, regardless of whether the analyzer quantifies IGs. On the other hand, there is significant interobserver variability in manually distinguishing between metamyelocytes and band neutrophils, with the latter best included in the neutrophil fraction and not separately reported, and less so by automated methods.
Barnes PW, McFadden SL, Machin SJ; International Consensus Group for Hematology. The International Consensus Group for Hematology review: suggested criteria for action following automated CBC and WBC differential analysis. Lab Hematol. 2005;11(2):83–90.
Bourne S, Ma N, Gulati G, Florea AD, Gong J. Evaluation of automated versus manual immature granulocyte counts. Lab Med. 2013;44(3):282–287.
Chabot-Richards DS, George TI. White blood cell counts: reference methodology. Clin Lab Med. 2015;35:11–24.
Eilertsen H, Hagve TA. Do the flags related to immature granulocytes reported by the Sysmex XE-5000 warrant a microscopic slide review? Am J Clin Pathol. 2014;142(4):553–560.
MacQueen BC, Christensen RD, Yoder BA, et al. Comparing automated vs manual leukocyte differential counts for quantifying the ‘left shift’ in the blood of neonates. J Perinatol. 2016;36(10):843–848.
Maenhout TM, Marcelis L. Immature granulocyte count in peripheral blood by the Sysmex haematology XN series compared to microscopic differentiation. J Clin Pathol. 2014;67(7):648–650.
Sireci A, Schlaberg R, Kratz A. A method for optimizing and validating institution-specific flagging criteria for automated cell counters. Arch Pathol Lab Med. 2010;134(10):1528–1533.
Alexandra E. Kovach, MD
Assistant Professor of Pathology,
Microbiology, and Immunology
Vanderbilt University Medical Center
Nashville, Tenn.
Member, CAP Hematology/Clinical
Microscopy Committee
 In this “Best of Q&A” series, we reprint select coagulation-related questions and answers. All have been chosen for their timeliness and relevance today. The following question and answer were published in August 2016.
In this “Best of Q&A” series, we reprint select coagulation-related questions and answers. All have been chosen for their timeliness and relevance today. The following question and answer were published in August 2016.
Q. Should a patient with a hematocrit greater than 55 percent be redrawn for correction always or only when prothrombin time and partial prothrombin time are elevated?
A. Accurate hemostasis and thrombosis results rely heavily on proper collection and processing (preanalytic phase) of the citrated blood specimen. Guidelines from many sources, including the Clinical and Laboratory Standards Institute,1 indicate that blood collection into nonactivating containers (e.g. polypropylene plastic or silicone-coated glass) with proper blood-to-anticoagulant ratio is required. Trisodium citrate tubes are available in a 3.2 percent or 3.8 percent concentration. A laboratory should choose a single concentration and not use the two citrate concentrations interchangeably.2 The World Health Organization and the CLSI recommend using 3.2 percent sodium citrate (105–109 nm/L), as the thromboplastin International Sensitivity Index values applied in the INR calculation are based on specimens collected in 3.2 percent citrate.2,3
The proper blood-to-anticoagulant ratio, commonly referred to as the “fill volume,” results in a 9:1 ratio of blood to anticoagulant. Underfilled tubes, defined as less than 90 percent of the fill volume, may result in prolongation of calcium-dependent, clot-based testing such as the PT and activated partial thromboplastin time (APTT) assays. Citrate’s anticoagulant effect is due to chelation of calcium in the specimen. When calcium is unavailable, coagulation cannot occur. During the analytic testing phase, a premeasured amount of calcium is added back, which allows coagulation to occur. If the citrate anticoagulant concentration is too high, the amount of calcium available during the testing phase is decreased, and the resulting time to clot formation is prolonged.
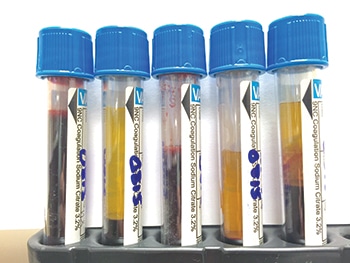
Underfilled sodium citrate tube. Citrate distributes only in plasma, and if a tube is underfilled, the reduced plasma volume will contain more citrate anticoagulant, leading to increased calcium chelation (see citrate tubes A–E, at right). Furthermore, there is an increased proportional volume of anticoagulant due to the lower plasma volume, which results in a potential dilution effect.2
The net effect is prolongation of clot-based assays (e.g. APTT, PT, protein C/protein S clot-based activity assays, and clot-based factor activity assays). The potential for erroneous results is often more pronounced in specimen tubes containing 3.8 percent sodium citrate or in smaller-volume containers such as half-draw or pediatric collection tubes.2,3
Hematocrit greater than 55 percent. Laboratories must also monitor for specimens with a hematocrit greater than 55 percent. In this situation, the plasma volume is reduced, resulting in a reduced plasma volume similar to that of an underfilled tube. The CAP hematology and coagulation checklist requires that laboratories have a written procedure for detection and special handling of specimens with elevated hematocrits.4 The amount of anticoagulant may require an adjustment in samples containing a hematocrit above 55 percent. The most efficient method to determine the appropriate citrate volume is to include a table in the laboratory specimen collection procedure indicating the modified volume of citrate for hematocrits greater than 55 percent. The formula to determine the correct volume of citrate for a given hematocrit is as follows5:
C = (1.85×10-3)(100−Hct)(V blood), where C indicates the volume (mL) of citrate needed in the tube; Hct (%), the hematocrit of the patient; and V, the volume (mL) of whole blood. Note: In a 3.5-mL specimen tube, the volume of blood drawn is 3.15 mL (i.e. V=3.15 mL in this equation).
In theory, should an underfilled tube or specimen with a hematocrit greater than 55 percent show normal screening PT or APTT coagulation results, one can conclude the patient has normal hemostatic results. However, this may be a deviation from standard operating procedure, so the medical director should make the final decision. Only the laboratory medical director or a qualified laboratory physician should approve deviations from an SOP. Before a laboratory physician approves the results from an improperly filled specimen collection tube, an investigation into the patient’s clinical situation and indication for testing should be reviewed. There are situations in which re-collection may pose increased risk to a patient (a neonate, for example). In such cases, performing the basic screening coagulation assays is indicated, and if the results are within normal limits, the laboratory physician may choose to release those results. Coagulation assays that do not rely on clot formation are often acceptable for testing, yet approval for testing should also be determined by the pathologist.
Other calcium-dependent, clot-based special coagulation assays, such as the protein C (PC) and protein S (PS) activity assays, which use PT or APTT methodology, should not be performed on an over-citrated specimen. In the PC and PS assays, falsely prolonged clotting times may result in overestimation of PC or PS activity. Thus, an over-citrated specimen secondary to an underfilled tube or hematocrit greater than 55 percent may be misinterpreted as having normal PC or PS activity. In the clot-based PC and PS activity assays, a short time to the clotting endpoint (fibrin formation) correlates to abnormally low PC and/or PS activity. Therefore, low PC and/or PS activity results from specimens that are underfilled or have hematocrit greater than 55 percent may represent a true, “qualitatively” low value, yet the accuracy (i.e. exact value) of the activity would be in question. If testing is performed, the pathologists must review these results and determine how (or if) the result should be reported. Clot-based factor activity assays are also subject to these preanalytic errors. Over-citrated specimens may cause falsely prolonged clotting times in the factor activity assays, resulting in erroneously low factor activity levels.
Overfilled sodium citrate tube. Overfilled specimen collection tubes can also occur. A common cause for overfilled specimen tubes is when whole blood is first drawn into a syringe and then forcibly injected into a specimen tube. Overfilled citrate tubes can also occur when the stopper (cap) is removed and additional blood is added. This may be an indication that a specimen from one collection tube was poured (added) into a second collection tube, and this practice is unacceptable.2 Overfilled tubes may result in poor mixing of the anticoagulant and lead to inaccurate results. Regardless of the cause of an overfilled tube, it violates the 9:1 ratio, and testing should be approved only by the pathologist.
In conclusion, improperly filled specimen tubes should call into question the collection process. The guidelines provided by CLSI H21-A5 clearly state, “Specimens that are clotted, collected in the wrong anticoagulant type (e.g., EDTA, sodium heparin), have other than a 9:1 blood to anticoagulation ratio, or are collected or stored in a container with an activating surface, are not suitable for testing and should be rejected [italics added].”1 One must be cautious when accepting an improperly collected specimen. Approving the specimen for testing often undermines the strict specimen-collection requirements designed for accurate coagulation test results and patient safety. Making exceptions to these rules may falsely reassure clinical medical providers that improperly filled citrate specimen tubes are acceptable. Exceptions to re-collection for underfilled tubes or patients with hematocrit greater than 55 percent should be considered only when screening PT and/or when APTT test results are normal, or when specimen re-collection is not possible.
- Clinical and Laboratory Standards Institute. Collection, Transport, and Processing of Blood Specimens for Testing Plasma-Based Coagulation Assays and Molecular Hemostasis Assays; Approved Guideline—Fifth Edition (H21-A5). Jan. 23, 2008.
- Kitchen S, Olson JD, Preston FE, eds. Quality in Laboratory Hemostasis and Thrombosis. 2nd ed. Chichester, West Sussex, U.K.: Wiley-Blackwell; 2013:45–56.
- Bennett ST, Lehman CM, Rodgers GM, eds. Laboratory Hemostasis: A Practical Guide for Pathologists. 2nd ed. Cham, Switzerland: Springer International; 2015:173–175.
- College of American Pathologists. Hematology and coagulation checklist. July 28, 2015.
- Kottke-Marchant K. An Algorithmic Approach to Hemostasis Testing. 2nd ed. Northfield, Ill.: CAP Press; 2016:46–47.
Andrew Jackson Goodwin IV, MD
Currently Associate Professor
Department of Pathology
University of Vermont
College of Medicine Burlington
Member of the CAP Coagulation Resource Committee at time of original publication