
Anne Ford
January 2015—If a picture is worth 1,000 words, what are 300 solid-organ transplant biopsy slides worth?
Don’t bother doing the math. No matter how you calculate it, the new Atlas of Transplant Pathology—which features more than 300 illustrations and is available this month from CAP Press—represents a wealth of concrete, up-to-date information on the pathologic diagnoses seen in heart, kidney, liver, lung, and pancreas transplants.

“In contrast to some other volumes that emphasize more of the underlying science and immunology, this really emphasizes the day-to-day routine diagnosis, and therefore it is user-friendly and it’s to the point,” says Philip T. Cagle, MD, who edited the volume with Lisa Yerian, MD, and Luan D. Truong, MD.
“It’s oriented in a practical way toward the surgical pathologist who receives these biopsies as part of routine patient care,” says Dr. Cagle, medical director of pulmonary pathology in the Department of Pathology and Genomic Medicine at Houston Methodist and professor of pathology and laboratory medicine at Weill Cornell Medical College of Cornell University.
With about 30,000 solid-organ transplants taking place in the U.S. each year, they have come a long way since the first successful kidney transplant was performed in 1954. More than 60 years later, “transplant patients have very good long-term outcomes, and they’re not necessarily sticking with their original transplant center for follow-up care,” says Dr. Yerian, director of hepatobiliary pathology at the Cleveland Clinic. “So they might be seen at a center that doesn’t do transplant pathology”—and where the pathologists on staff may not have a great deal of firsthand experience with transplanted organs.
Experienced or not, Dr. Cagle says, those pathologists “may be called upon to do a number of things, including look at donor organs before they are sent to a location where they will be transplanted into a patient. Or they may be asked to look at biopsies for infections and other relatively common problems that transplant patients encounter.”

“There are going to be more biopsies from these transplanted organs, because not infrequently these organs do not function well,” agrees Dr. Truong, medical director of nephropathology in the Department of Pathology and Genomic Medicine at Houston Methodist and professor of pathology and laboratory medicine at Weill Cornell.
That’s where a resource such as the Atlas of Transplant Pathology comes in.
The atlas’ sections on liver donor organ evaluation (to be published in full next month) and lung-transplant–associated infections are likely to be of particular value to pathologists who do not work at transplant centers, Dr. Cagle says. “For example, as a pathologist who does not specialize in liver pathology, I have to evaluate liver donor organs all the time. Likewise, pathologists everywhere look at biopsies for infections in lung transplant patients, even those in community hospitals who do not specialize in transplant pathology.”
The organization of those sections, as well as the rest of the atlas, is likely to appeal most to what one contributor calls “splitters”—pathologists who prefer to partition their diagnoses, rather than “lumpers,” who tend to cluster them.
“This particular book is going to be useful for those who like to split things and understand them separately, rather than read an entire chapter and then clarify those fine lines of division in their mind,” says E. Rene Rodriguez, MD, who helped write the section on heart transplantation and who is section head of cardiovascular pathology at the Cleveland Clinic.

“In other atlases,” he adds, “the chapter on heart transplantation would go into a little history, give a few concepts and discuss how those concepts have changed, and then show you everything about the heart, starting with cellular rejection, antibody-mediated rejection, cardiac allograft vasculopathy, etc.—all that in one chapter that goes on for page after page.”
In contrast, the Atlas of Transplant Pathology’s heart transplantation section consists of eight subsections, each of which addresses a single concept, such as endomyocardial biopsy for transplant evaluation, antibody-mediated rejection, and recurrent disease in the transplanted heart. “It’s very easy to pick up any chapter independently from another and understand it very clearly, even though the spectrum of the rejection process, for example, is not black and white; in some patients it is rather gray. But if you put all the information in one place, it’s a little harder for the reader to digest it quickly and go through it,” Dr. Rodriguez says.
Then, too, the concept-by-concept format may make it easier for readers to take in the newest, most up-to-date information contained in the atlas, such as the material on antibody-mediated rejection in heart transplants. “Up until less than five years ago, surgeons, cardiologists, and even pathologists questioned whether that was an issue that affected the patient,” Dr. Rodriguez says. “And there were no unified criteria on how to diagnose it. In the last few years, the International Society for Heart and Lung Transplantation finally came up with criteria on how to diagnose antibody-mediated rejection in heart in a standard way. That’s the part of the heart section that will make anybody grabbing this atlas say, ‘Oh, wow, this is current knowledge.’”

Other sections of the atlas, too, contain new information on antibody-mediated rejection. “This is a critical area in transplant pathology, and over the past few years there have been several seminal studies that have provided novel insights into this pathologic process,” says Dr. Truong, who contributed to the kidney section. These new findings are incorporated into the updated Banff Classification of Renal Allograft Pathology published in 2014, he says, “leading to revised and improved diagnostic criteria, together with their practical applications in renal transplant biopsy interpretation. These important developments are thoroughly reviewed in various chapters of this atlas.”
Dr. Cagle and his co-editors were nearing completion of the atlas’ manuscript when, in April 2014, the meeting report of the Banff Conference on Allograft Pathology was issued. “The Banff report is based on a consensus conference of transplant experts and updates criteria for rejection classification and other recent advances,” Dr. Cagle says. “Findings in this report were taken into account in revising our manuscript.”
One newly described entity that appears in the lung section of the atlas: restrictive allograft syndrome. “The main pathologic finding is fibroelastosis of the visceral pleura,” Dr. Cagle explains, “which hampers the ability of the lung to expand and exchange gas. We have some other findings that we can see as well, but that’s the one that sets this apart, and it’s something that might not be fully appreciated by pathologists if they’re not aware of this.”
Among the other sections of the atlas that contain newly described entities or other new findings are: in heart, cardiac allograft vasculopathy; in kidney, glomerulitis and transplant glomerulopathy; in liver, donor organ evaluation, preservation injury, and antibody-mediated rejection; and in lung, lung-transplant–associated infections and lung-transplant–associated organizing pneumonia.
To Dr. Yerian, the value of the atlas rests in large part on its illustrations. “We wanted to provide enough text to be informative, but not an extensively detailed, heavily referenced discussion on each topic, because that’s already available out there,” she says. “We just wanted enough text to support an interpretation of the pictures. The pictures are the magic of what we do.”
How so? Well, “one of the things I observe as a liver pathologist is that acute rejection doesn’t always look like the same thing; it’s not a picture-matching diagnosis, where if you see it once, you always recognize it,” she says. “There’s quite a spectrum of appearances. So what we try to do in the atlas is give a sense of the spectrum of morphology you can see with any given entity. In many cases, the reader will find more than one picture of a given entity, to really try to illustrate the spectrum of changes you can see. You can list the features, but that’s not going to get you far enough; you need to see the spectrum of changes, because there are subtleties in the morphology that we’re just not great at articulating with words yet. We aim to see as many examples, as much of the spectrum as possible, in order to better understand what an entity is and, even more importantly, what it isn’t.”
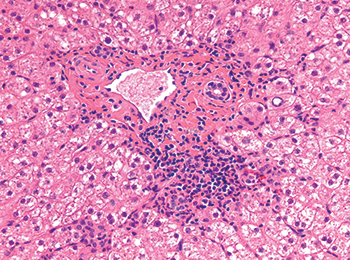
One such spectrum: the many patterns of immune-mediated graft injury that may be seen in transplanted livers, “including patterns that have more prominent centrilobular distribution,” she says. “Plus, there’s variation among patients. Some might have more prominent bile duct damage, whereas endotheliitis might be more prominent in others.”
Then, too, she continues, “In early acute rejection episodes, you commonly see a prominent mixed portal infiltrate with very large, active appearing lymphocytes. But as time progresses, we can see an evolution toward a more mononuclear infiltrate, more mature and lymphocyte-predominant, and more reminiscent of a chronic hepatitis pattern. That’s a really common and important diagnostic problem.”
[hr]
Anne Ford is a writer in Evanston, Ill. To order a print book (PUB124), go to www.cap.org (“Shop” tab) or call 800-323-4040 option 1. For members, $76; for nonmembers, $95. To order an ebook, go to ebooks.cap.org ($65).