 CAP TODAY Pathology/Laboratory Medicine/Laboratory Management
CAP TODAY Pathology/Laboratory Medicine/Laboratory Management


Fig. 3.1.6. Moderate macrovesicular steatosis (30%–60%). Although this liver contains greater than mild steatosis, it may be considered acceptable for use in selected settings.
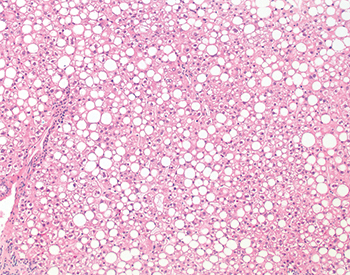
Fig. 3.1.7. Severe macrovesicular steatosis (>60%). This graft was found to be severely steatotic (80% steatosis overall) on routine time-zero biopsy; no frozen section was performed prior to implantation. Although in this case the organ functioned well and the recipient experienced a normal posttransplant recovery, severely steatotic livers would not be used in most settings if detected prior to implantation.
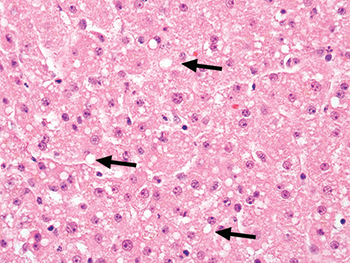
Fig. 3.1.8. Small droplet steatosis. This previously frozen biopsy demonstrates scattered small fat droplets (arrows) that neither fill the cell nor displace the nucleus. These droplets resolve after implantation of the liver and do not impact graft function.
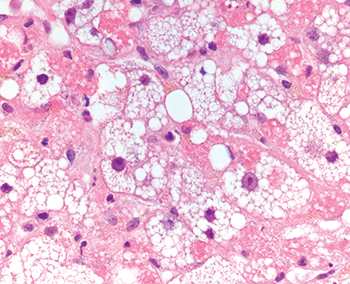
Fig. 3.1.9. Microvesicular steatosis. Numerous tiny fat droplets surrounding the hepatocyte nucleus impart a foamy or finely vesicular appearance to the hepatocyte. This change is rare in livers being evaluated for potential transplantation.
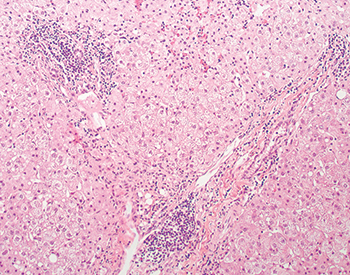
Fig. 3.1.10. Chronic hepatitis. Portal inflammation is seen in this hepatitis-C–positive “extended-criteria” donor. This finding is expected and is not a contraindication to use of this organ in selected clinical settings.
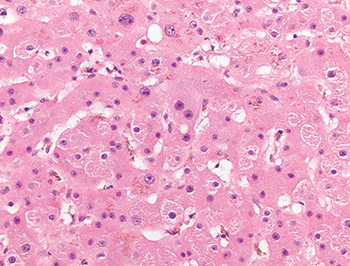
Fig. 3.1.11. Iron overload in donor liver. Hepatocellular and sinusoidal iron pigment is evident on the hematoxylin-eosin (H&E)–stained slide in this donor liver biopsy.
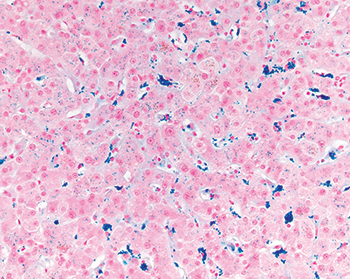
Fig. 3.1.12. Iron overload in donor liver, Prussian blue stain. A Prussian blue stain performed on the biopsy illustrated in Figure 3.1.11 confirms mild iron accumulation in hepatocytes and Kupffer cells.