
Desiree Marshall, MD; Dhruba J. SenGupta, PhD; Daniel R. Hoogestraat, MB(ASCP); Karen Stephens, PhD; Brad T. Cookson, MD, PhD; Cecilia C.S. Yeung, MD
![]() February 2013—CAP TODAY and the Association for Molecular Pathology have teamed up to bring molecular case reports to CAP TODAY readers, starting this month. AMP members will write the reports using clinical cases from their own practices that show molecular testing’s important role in diagnosis, prognosis, treatment, and more. We aim to publish a few a year. The first such report comes from the University of Washington Medical Center, Seattle. (If you would like to submit a case report, please e-mail the AMP at amp@amp.org. For more information about the AMP, visit www.amp.org.)
February 2013—CAP TODAY and the Association for Molecular Pathology have teamed up to bring molecular case reports to CAP TODAY readers, starting this month. AMP members will write the reports using clinical cases from their own practices that show molecular testing’s important role in diagnosis, prognosis, treatment, and more. We aim to publish a few a year. The first such report comes from the University of Washington Medical Center, Seattle. (If you would like to submit a case report, please e-mail the AMP at amp@amp.org. For more information about the AMP, visit www.amp.org.)
Abstract
Zygomycoses are morbid and often fatal diseases. We report a case of unexpected primary gastrointestinal zygomycosis presenting as small bowel obstruction with a palpable abdominal mass in a marrow transplant patient. This patient incurred a rapidly fatal hospital course, and subsequent autopsy findings showed ambiguous histologic features in the fungus requiring molecular identification. The case demonstrates the importance of recognizing zygomycosis as a rapidly fatal process in an immunocompromised patient despite the unusual presentation. It also highlights the utility of gene sequencing in a postmortem setting for speciation of fungal organisms, both for providing a definitive diagnosis and additional information for infection control.
Introduction
Zygomycosis is the third most common invasive fungal infection, representing 8.3 to 13 percent of fungal infections at autopsy in hematology patients.1 Mucorales fungi, which cause the majority of human disease, are an order of Zygomycetes and include the genera Rhizopus and Mucor. They are ubiquitous and cause acute angioinvasive infections in immunocompromised patients.1 Many institutions have shown increased frequency of zygomycosis attributed to increased use of immunosuppressive drugs and antifungal therapy lacking activity against Mucorales (for example, voraconazole).1,2 Populations at risk include patients with hematologic malignancies, diabetes mellitus, prolonged neutropenia, solid organ transplant, iron overload/deferoxamine therapy, major trauma, prolonged use of corticosteroids, illicit intravenous drug use, neonatal prematurity, and malnourishment.2
We report a case of unexpected, rapidly fatal primary gastrointestinal zygomycosis presenting as small bowel obstruction with a palpable abdominal mass in a marrow transplant patient. Subsequent autopsy findings required molecular testing by gene sequencing to identify the organism. We report this case for the purpose of recognizing a rapidly fatal process in an immunocompromised patient and to describe the utility of molecular methods in speciation of fungal organisms in a postmortem setting.
Patient case
A 67-year-old man with transformed diffuse large B cell lymphoma from follicular lymphoma was admitted with severe mucositis and nausea/vomiting four days following autologous peripheral stem cell transplant. His past medical history was significant for insulin-dependent type 2 diabetes mellitus complicated by renal insufficiency, atrial fibrillation, hypertension, hypothyroidism, and colonization by vancomycin-resistant enterococci (VRE). Social and family history included distant work on nuclear submarines and a sister in remission from follicular lymphoma. Upon admission, he was on a prophylactic regimen of levofloxacin, fluconazole, and acyclovir. He developed neutropenic fever on hospital day two with absolute neutrophil count (ANC) of 0/mm3, and levofloxacin was changed to ceftazidime. That evening he had an episode of bilious vomiting, suspicious for small bowel obstruction. Two days later, he demonstrated neutrophil engraftment with ANC of 800/mm3, but also developed atrial fibrillation with rapid ventricular response and underwent cardioversion. Abdominal CT revealed small bowel dilation and wall thickening with extensive mesenteric fat stranding and enlarged retroperitoneal lymph nodes. The differential diagnosis included ischemia secondary to embolic event, infection, recurrent lymphoma, chemotherapy-related toxicity, graft-versus-host disease, or vasculitis.
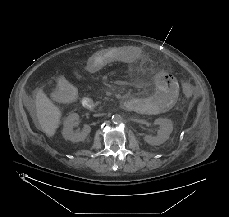
His multiple comorbidities made him a poor surgical candidate, and conservative management with the addition of metronidazole was initiated on hospital day four. Although he showed initial improvement, his abdominal symptoms progressively worsened. He had a heme-positive bowel movement on hospital day 14 with stool culture negative for Clostridium difficile and Norovirus; planned additional studies were not performed due to insufficient material. Repeat abdominal CT on hospital day 15 showed progression of the abdominal process (Fig. 1). The next day he had blood per NG tube, left upper quadrant ecchymosis, increased abdominal distension, and an underlying palpable mass. He continued to decompensate until hospital day 18 when he died after unsuccessful resuscitative efforts for bradycardia, acute hypotension, and acidosis.

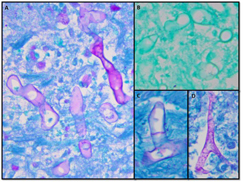
Autopsy revealed a large, complex pseudocavitary lesion formed by necrotic omentum encasing several necrotic loops of small bowel with partial entrapment of the transverse colon and two large necrotic abscess cavities in the mesentery and below the stomach. A definite perforation was not identified by gross examination. A large annular, hemorrhagic, necrotic lesion corresponded to the superficial ecchymosis on the left upper to mid quadrant abdominal skin (Fig. 2). Microscopic examination of involved tissues revealed extensive infiltration by PAS-positive, GMS-negative fungal organisms with prominent angiotropism. Some fungal forms showed Zygomycetes morphology with aseptate, ribbon-like hyphae of variable width (Fig. 3). However, some hyphae showed features not typically associated with Zygomycetes, including septa formation, narrower hyphae, and 45-degree angle branching (Fig. 3). Postmortem viral, bacterial, and fungal cultures from the omentum, brain, spleen, liver, kidney, right and left lungs, peripancreatic necrosis, and retro-gastric abscess revealed no evidence of disseminated fungal infection; however, the lungs, omentum, kidney, liver, and brain grew Enterococcus species. Extensive sampling of the tissues showed no lymphoma.
Due to ambiguous fungal morphology, PCR analysis of formalin-fixed paraffin-embedded tissue from the peripancreatic necrosis and retro-gastric abscess was performed with methods reported previously.3 PCR products were separated by electrophoresis using a one percent agarose gel. PCR using primers directed against internal transcribed spacer (ITS1) yielded a product that was subjected to bidirectional sequencing and contig assembly. Assembled sequence was submitted to GenBank Basic Local Alignment Search Tool (BLAST) search. The query sequence matched 100 percent over 312 base pairs to Rhizopus microsporus (GenBank accession No. DQ119009) and Rhizopus azygosporus (GenBank accession No. DQ119008) sequences (Fig. 4).
Discussion
Zygomycoses are classified into six major clinical forms, including rhinocerebral, pulmonary, cutaneous, gastrointestinal, disseminated, and uncommon presentations. Gastrointestinal zygomycosis is uncommon, with only 25 percent of cases being diagnosed premortem because of its nonspecific presentation. This leads to frequent delay in diagnosis and a mortality rate of 85 percent.2 The stomach is most commonly involved, often with gastric perforation, followed by the ileum and cecum with presentation involving an appendiceal, cecal, or ileal mass.2
In our case, ischemia, infection, and recurrent lymphoma were high on the list of differential diagnoses. Although a single stool sample was negative for Clostridium difficile and Norovirus, specimen limitations precluded additional studies. In the absence of specific findings, the patient was maintained on broad-spectrum antibiotics and prophylaxis with fluconazole. Azoles generally lack activity against Zygomycetes.1 Amphotericin B is the agent of choice for most Mucorales, although its efficacy is variable depending on the specific organism.1 A second case of zygomycosis occurred in our institution, also requiring molecular identification, and was shown to be the same species as in this case. However, because of the lack of a pure culture specimen, further testing for infection control studies proved to be challenging. A recent study describing an outbreak of gastrointestinal zygomycosis due to Rhizopus microsporus had patients who presented with segmental bowel thickening and intra-abdominal abscess formation; however, the spectrum of clinical manifestation ranged from asymptomatic mucosal colonization to invasive disease.4
Diagnosing zygomycosis is difficult because tissue culture is often negative.5 Although the gold standard for diagnosis is histologic examination, fungal morphology, even aided by special stains (PAS and GMS), is unreliable5 for use as the only means of identification. There is a chance for incorrect diagnosis if adequate fungal hypha or the classic morphology is not seen. In addition, microscopy cannot differentiate fungi beyond the genera level. Fluorescent antibody staining and newer immunohistochemical methods have shown improved identification over conventional modalities (H&E and special stains); however, these methods are not yet widely used.5 Culture-independent nucleic-acid based methods such as PCR are rapid and sensitive and can be used on fresh or formalin-fixed tissue. Targeting of multi-copy loci, particularly the ribosomal DNA genes (18S, 28S, and 5.8S) and the intervening internal transcribed spacer (ITS) regions (ITS1 and ITS2), allow increased specificity with identification to the species level.6 Such specificity is important in selecting appropriate antifungal therapies.
With the high mortality rates of invasive fungal infections, the autopsy becomes an important tool to study the patterns and prevalence of such infections. It provides key information for hospital QA/QC and has the potential to identify emerging infections. In addition, unexpected diagnoses from autopsy provide valuable learning experiences, such as the need to maintain a high degree of suspicion for zygomycosis in vulnerable patient populations, as exemplified in this case. Molecular microbiology techniques have proved to be a significant source of data for these purposes. The information gained will better equip clinicians to manage these devastating infections.
Conclusion
This case emphasizes the importance of including zygomycosis in the differential diagnosis, especially in immunocompromised patients with unusual presentations and multiple risk factors. As fungal culture can be insensitive and morphology can be unclear, molecular techniques are critical tools in the diagnosis and selection of therapy for these cases. Using such techniques in the postmortem setting can aid in infection control and in understanding disease epidemiology, with the potential for improving outcomes in future patients.
References
- Prabhu RM, Patel R. Mucormycosis and entomophthoramycosis: a review of clinical manifestations, diagnosis, and treatment. Clin Microbiol Infect. 2004;10(suppl 1):31–47.
- Petrikkos G, Skiada A, Lortholary O, et al. Epidemiology and clinical manifestations of mucormycosis. Clin Infect Dis. 2012;54(suppl 1):s23–s34.
- Harrington AT, Creutzfeldt CJ, SenGupta DJ, et al. Diagnosis of neurocysticercosis by detection of Taenia solium DNA using a global DNA screening platform. Clin Infect Dis. 2009;48:86–90.
- Cheng VCC, Chan JFW, Ngan AHY, et al. Outbreak of intestinal infection due to Rhizopus microsporus. J Clin Microbiol. 2009;47(9):2834–2843.
- Sangoi AR, Rogers WM, Longacre TA, et al. Challenges and pitfalls of morphologic identification of fungal infections in histologic and cytologic specimens: a ten-year retrospective review at a single institution. Am J Clin Pathol. 2009;131:364–375.
- Munoz-Cadavid C, Rudd S, Zaki SR, et al. Improving molecular detection of fungal DNA in formalin-fixed tissues: comparison of five tissue DNA extraction methods using panfungal PCR. J Clin Microbiol. 2010;48(6):2147–2153.
Dr. Marshall is a PGY3 resident in anatomic pathology, Dr. SenGupta is a research scientist in laboratory medicine, Dan Hoogestraat is a laboratory technologist in laboratory medicine, Dr. Stephens is a professor of laboratory medicine, Dr. Cookson is a professor of laboratory medicine, and Dr. Yeung is an assistant member at Fred Hutchinson Cancer Research Center and an acting assistant professor in anatomic pathology—all at the University of Washington, Seattle.
Test yourself.
Here are a few take-home points and questions. Answers to the questions are online now at www.amp.org/casereviews and will be published in CAP TODAY next month.
1. Zygomycoses are important to recognize and treat aggressively in immunocompromised patients due to a highly morbid and often fatal clinical course.
Which statement is false?
a) Zygomycosis may cause a rapidly fatal, clinically obscure infection even in non-immunocompromised patients.
b) As a class of antifungals, azoles have good efficacy against Zygomycetes.
c) The stomach is the most common site of infection in gastrointestinal zygomycoses.
d) Zygomycoses may infect a wide range of tissue sites, possibly leading to uncommon presentations that evade early detection.
2. In tissue, zygomycosis may show variation from normal characteristic morphology (variable-width ribbon-like hyphae, irregular branching, aseptate), but are typically PAS positive and silver negative.
Classic Zygomycete morphology includes:
a) 45-degree branching.
b) Narrow filamentous hyphae.
c) Budding yeast forms.
d) Fruiting bodies.
e) No to weak reactivity with silver special stains.
3. Molecular identification of organisms in paraffin-embedded tissues is a rapid and accurate diagnostic test, and if done in a timely manner, can guide clinical therapies.
Which diagnostic modality cannot identify fungal organisms beyond the genera level?
a) Fungal culture.
b) Ribosomal DNA sequencing.
c) Histomorphology and special stains.
d) MALDI-TOF mass spectrometry.