
Amy Carpenter Aquino
March 2023—When it comes to molecular syndromic panels for pneumonia, there’s both upside and downside, says Neil W. Anderson, MD, D(ABMM), associate professor, Department of Pathology and Laboratory Medicine, Washington University School of Medicine in St. Louis.
They’re fast, easy, and close to comprehensive for potential pathogens, and they can detect some culture-negative infections. On the other hand, there are gaps in the panels—particularly for novel pathogens, and a poor-quality specimen for culture is also a poor specimen for PCR. And the panels aren’t standalone tests, “no matter how you cut it,” Dr. Anderson says. “You have to still grow these organisms to confirm identification and to perform phenotypic susceptibility.”
“This isn’t the be-all and end-all, the one test for patients with pneumonia. But it’s a little closer to that,” he said in an AACC session last year, in which he described his laboratory’s implementation of a pneumonia panel. He is medical director of the molecular infectious disease laboratory and assistant medical director of the microbiology laboratory at Barnes-Jewish Hospital. “Implementation of this testing was an intricate process for us,” he said.
Clinical outcome and impact studies to date are few, he noted, but the potential value of pneumonia panel testing, which includes detection of resistance markers, is significant. In his laboratory, since he and colleagues went live with panel testing in 2021, they have seen anecdotally a potential for antimicrobial escalation and use of infection prevention measures if a carbapenemase-associated gene is detected.
Antimicrobial deescalation or avoidance is quite likely, thanks to the high negative predictive value for on-panel organisms. A study published last fall, using the Uny-vero pneumonia panel (Curetis, Germany), which is FDA cleared for tracheal aspirate and broncho-alveolar lavage samples, found the testing to decrease the duration of inappropriate antibiotic therapy of patients admitted to the hospital with pneumonia and at risk of Gram-negative rod infection (Darie AM, et al. Lancet Respir Med. 2022;10[9]:877–887). The multicenter, randomized controlled trial was conducted at two tertiary care centers in Switzerland.

“They took 208 patients and divided them into a PCR group or a conventional microbiology group. The patients then received antimicrobials per the treating physician,” Dr. Anderson said. For the PCR group, results were reported directly to pharmacy colleagues within five hours, accompanied by written guidance for appropriate therapy and considering local resistance rates, he noted. “A very active way of reporting.”
The overall duration of inappropriate antimicrobial use in the PCR arm was shorter by 38 hours (47.1 versus 85.7, P<0.0001). “Definitely showing an impact here,” Dr. Anderson said. “Interestingly, there was no difference in time to discharge.”
Multiple diagnostic tests and methods are required for a comprehensive evaluation for pneumonia, ranging from antigen-based to culture-based to molecular testing. “Sometimes even direct observation of specimens is necessary to give us a clue of the pathogen and inform downstream testing,” Dr. Anderson said. These methods by themselves have severe limitations—many are narrow. The broader methods such as culture are more time-consuming and may not provide an answer quickly enough. Direct observation and staining can identify more but be difficult to interpret. “A lot of us aren’t going to make a diagnosis of a specific pathogen based merely on the direct stain.”
Multiplex panels have been used to diagnose pneumonia for some time. “A lot of laboratories are using the upper respiratory panels that target a variety of atypical bacteria and viruses and using those in an off-label way—we validate this, of course—on lower respiratory specimens to at least have some sort of multiplex testing on these specimen types.”
With the dedicated pneumonia panels, he said, “we’re testing for what we all refer to as ‘regular’ bacteria” that could be part of normal flora, and there are two ways to do so: providing a semiquantitative result—“telling the provider how much is there”—and using positivity cutoffs that may be more applicable to relevant quantities. The resistance markers that these newer methods detect predict resistance but not necessarily susceptibility, he said.
The Unyvero lower respiratory panel is “sample to answer,” Dr. Anderson said, but a separate instrument is needed for extraction, amplification, and detection. Its run time is less than five hours—“not incredibly fast but quicker than a culture”—and it provides a qualitative detection for all targets. A CE version provides semiquantitative readouts for bacterial targets, but the FDA-cleared version is qualitative. The panel targets 20 microorganisms (19 bacterial, one fungal) and 10 resistance markers (Sun L, et al. Eur J Clin Microbiol Infect Dis. 2021;40[10]:2113–2121; Collins ME, et al. J Clin Microbiol. 2020;58[5]:e02013-19; Klein M, et al. J Clin Microbiol. 2021;59[3]:e02497-20).
For the BioFire FilmArray pneumonia panel, sputum, tracheal aspirate, and bronchoalveolar lavage specimen types have been cleared. The panel targets 15 bacteria and seven antimicrobial resistance genes. “We also have different viruses and atypical bacteria” not on the Unyvero panel, he said, many of which are common to the BioFire upper respiratory panel.
The panel’s semiquantitative reporting applies to 15 common colonizers. “There’s a comparison of the target to an internal quantified standard,” Dr. Anderson explained, “and this is used to extrapolate copies per mL, and the copies per mL are reported into semiquantitative bins.” A value of 4 × 105 copies per mL would simply be reported as being in the 105 bin, for example, “so you’re not getting an exact quantification,” he said, noting results are similar to those expected from culture. Antimicrobial resistance genes are tested for qualitatively and reported only if a compatible organism is present.
The Unyvero and BioFire panels “do a good job of covering the bacterial causes of community-acquired pneumonia,” and the BioFire panel also covers the common causes of community-acquired viral pneumonia, Dr. Anderson said, adding the data his laboratory reported were gathered pre-COVID (Webber DM, et al. J Clin Microbiol. 2020;58[7]:e00343–20). Both panels adequately cover the common bacteria that cause hospital-acquired pneumonia, he said, but Stenotrophomonas maltophilia, accounting for three percent of cases, is present only on the Unyvero panel.
In evaluating the BioFire panel at Barnes-Jewish Hospital, his group used 200 consecutively available lower respiratory tract specimens from ED and ICU patients submitted for standard-of-care testing. “Every one of these specimens had a lower respiratory tract culture performed, so they all had bacterial culture, but they may have had different viral testing as well.” They tested the remnant samples using the pneumonia panel and compared the results with the standard-of-care testing. They detected a bacteria or virus in 58.5 percent (117/200) of specimens. “A lot of positives,” Dr. Anderson said, “and a lot of dual positives or positive specimens with three, perhaps even four, targets.” Multiple targets were detected in 43 percent (50/116) of the positive specimens.
A European multicenter study of 2,476 specimens from 52 laboratories had similar findings (Ginocchio CC, et al. Eur J Clin Microbiol Infect Dis. 2021;40[8]:1609–1622). “Their results line up to ours pretty well,” Dr. Anderson said. A bacteria or virus was detected in 75 percent of specimens, and more than one pathogen was detected in 46 percent of positive specimens. “So it’s safe to say the literature confirms you will get a lot of positivity with an assay like this,” he said.
For viral targets, Dr. Anderson and colleagues found the pneumonia panel performs well compared with their standard-of-care viral testing. They did a separate analysis of remnant specimens from the 200 specimens and tested them also by the BioFire upper respiratory panel (RP2.0), “and the comparison was nearly exact,” with 96 percent concordance, he said. For something like flu or RSV, “the testing with the pneumonia panel versus the upper respiratory panel is essentially equivalent. So you don’t need both” (Hughes AEO, et al. J Clin Microbiol. 2020;58[6]:e00254-20).
The panel missed eight instances of bacterial detection by the standard-of-care method because the targets weren’t included on the panel, Dr. Anderson said, with Stenotrophomonas maltophilia accounting for about 50 percent of the misses.
There were 92 instances of unique pneumonia panel detections that were not reported from the culture-based testing; 22 were Staphylococcus aureus, and 25 were Haemophilus influenzae. “We know these are part of normal flora,” so the panel could have detected something the laboratory didn’t report out in culture but was part of normal flora, “or maybe it was detecting flora that never actually grew on the plate,” he said.
Many detections of Streptococcus pneumoniae are unique to the panel, Dr. Anderson said, noting the organism doesn’t grow well in culture if a patient has had an antimicrobial pre-culture. “And these could potentially be clinically relevant, molecular-only detections that we’re going to miss with our culture-based techniques.”
The findings of Ginocchio, et al., reported in 2021, “almost exactly mimic ours,” he said, in their many instances of unique pneumonia panel detections for S. aureus, H. influenzae, and S. pneumoniae. His own group’s data reveal these detections are linked to lower organism load. If the pneumonia panel was 104 or 105, “it’s far less likely that we’re going to recover that in culture. Either it’s going to be interpreted with the mix, or it just isn’t going to grow,” he said. They found, too, that for S. aureus, the unique detections are more common in potentially polymicrobic specimens, such as sputum-type specimens. “Not surprising,” he said, “because the hypothesis is that we’re detecting it in the normal flora,” and specimens that have more normal flora will have more unique detections.
Once the panel is implemented, Gram stain triage still plays an important role. “We all know garbage in, garbage out,” Dr. Anderson said. “If you have a specimen that’s loaded with squamous epithelial cells, it’s probably oral contamination. We’ve already seen those extra detections associated with sputum-like specimens,” all of which were acceptable for testing. “You can imagine it would be far worse if we had a lot of orally contaminated specimens,” which is why the triage is important. His laboratory rejects all specimen types and samples with excessive squamous epithelial cells for multiplex molecular syndromic pneumonia panel testing, and has always done the same for culture from sputum-type specimens.
Because Gram stain plays an important role, “it’s going to complicate your workflow, because unlike a lot of your molecular testing, you can’t just send it off to the molecular lab and have it tested,” he said. Gram stain triage has to come first, and “with that triage comes communication.” Even though the microbiology and molecular laboratories at Barnes-Jewish are across the hall from one another, “there are still challenges with communicating whether the testing needs to be done” and how to hand off the specimen.
Their solution: A stickered sheet with the patient’s information accompanies the specimen to the microbiology laboratory, and on it they check whether the Gram stain was acceptable. Whether the specimen will go for molecular testing and culture, or culture only, or neither is also accounted for on the sheet, “and it tells our technologists exactly what to do,” Dr. Anderson said.
Rejected specimens are reported in the EHR with a note: “Abundant squamous epithelial cells observed on Gram stain. Specimen will not be processed for molecular analysis.”
Gram stain and culture must accompany an order for panel testing, and the order set also includes SARS-CoV-2, which is absent from the panel. “There’s a lot of discussion about how these should be offered together,” he said. The panel is orderable as pneumonia PCR with aerobic culture and Gram stain. For patients with cystic fibrosis there is a special pulmonary culture order. “The bacteria included on these panels are not the same bacteria, or many of the same bacteria, that cause disease in cystic fibrosis patients,” he explained, “so it’s not an appropriate test for that patient population.”
Ordering is otherwise unrestricted, Dr. Anderson said, though a soft stop alerts providers if a repeat pneumonia panel has been ordered within three days to curb repeat testing. This extends to repeat viral testing, such as a flu-positive result from the prior day or concern about viral pneumonia. It’s redundant to test for both, “so we let them know that that testing’s already occurred and ask if they wish to proceed.”
They report all detections with semiquantitative values and use no specimen type thresholds. “We report it as it comes off. But we do not report the data in its raw form,” because a report scanned into a patient chart would be difficult for providers to interpret. For upper respiratory panels, providers are accustomed to receiving all viral and atypical bacterial targets in a listed format. “And half of this panel is the upper respiratory panel, so we want to be able to maintain that to some degree,” Dr. Anderson said. “But we also want to maintain the cultural context for those bacterial targets. They need to be interpreted with the culture, and we wanted to make sure that was linked.” The laboratory therefore reports all atypical bacteria and viruses in a list.
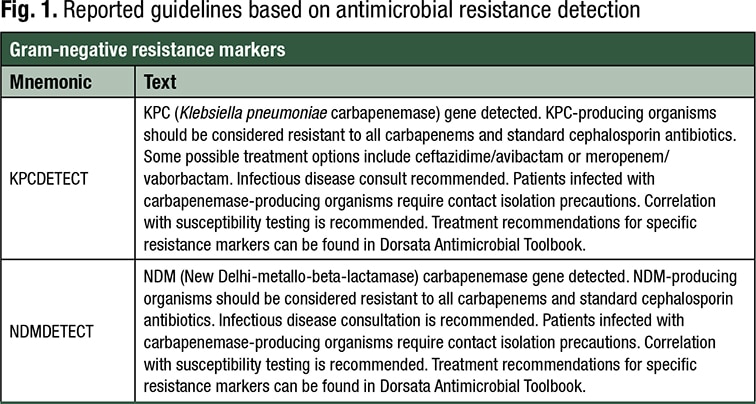
Bacteria and antimicrobial resistance targets are reported as a narrative within the corresponding culture report, including the presence, not absence, of Gram-negative resistance targets. “So we’re not saying, ‘It’s negative for resistance,’ because these are much better at predicting resistance than susceptibility,” he said. “We don’t want someone to look at absence as ‘Now I can use a less broad-spectrum drug.’” Interpretive notes are provided (see examples in Fig. 1).
Adding action to the results is important. “You can’t just plop this down and expect your providers to act on it,” Dr. Anderson said. Guidance is needed. At Barnes-Jewish, pharmacy, infectious disease, and laboratory leaders wrote a guide on what to do with results and distributed it electronically. “It gives our providers a road map to these results they’re not used to seeing.”
Amy Carpenter Aquino is CAP TODAY senior editor.