 CAP TODAY Pathology/Laboratory Medicine/Laboratory Management
CAP TODAY Pathology/Laboratory Medicine/Laboratory Management

“Understandably, in some situations, older archived specimens may be all that is practically available to you, but when possible, fresh cut slides from those stored blocks should be used.”
Fixation methods and cold ischemic times are preanalytic factors. Fixation time has to be within six to 72 hours. Numerous published studies have shown that tissues subjected to prolonged cold ischemic time can yield false-negative biomarker results. “I do think this issue may be exacerbated when we consider tumors with subtle expression or on the lower spectrum of HER2 expression,” he said.
Differences in the assay itself are a factor. Several FDA-approved assays are cleared for HER2 IHC assessment, but they use different antibodies, have different detection and retrieval systems, and have different performance characteristics, Dr. Tozbikian noted. At OSU, rabbit monoclonal 4B5 is used, but he encounters different HER2 IHC on the department’s consult service.
“I see cases where biomarkers are done at outside labs, and when you look at them, the stains look different in intensity, staining quality, and background. For these assays, while analytic validation and agreement have been well studied in identifying HER2-positive disease, a lot less is known about their comparative performance in detecting tumors with lower levels of HER2 expression. That’s something we all need to bear in mind going forward.”
The 3+ HER2 positive result is defined as circumferential membrane staining that is complete and intense in more than 10 percent of tumor cells. With different assays they look different (Fig. 1).
A 2+ result is defined as weak to moderate complete membrane staining observed in more than 10 percent of tumor cells (Fig. 2). “Less common staining patterns that are also considered 2+ include incomplete basolateral staining that is seen in, say, micropapillary tumors or intense complete staining that is seen in less than 10 percent of the tumor cells. And these would require reflex HER2 ISH for arbitration.”
A HER2 negative score of 1+ is defined as incomplete membrane staining that is faint or barely perceptible and observed in more than 10 percent of tumor cells (Fig. 3). A 0 score is defined as a complete absence of staining or incomplete, faint, barely perceptible staining seen in less than or equal to 10 percent of the invasive tumor cells (Fig. 4).
Making the distinction at the lower end of the spectrum of HER2 expression requires careful examination of the entire tumor, Dr. Tozbikian said. He recommends initially scanning the tumor at low magnification to evaluate for that presence of intratumoral heterogeneity. “To be able to detect low levels of HER2 expression requires that the pathologist carefully interrogate the tumor at higher power. There’s simply no avoiding this. It can’t be done at scanning magnification alone,” he said. In 2+ cases, the staining precipitates generally start to become visible at medium power using the 10× objective lens, “but to observe 1+ staining requires the pathologist to go to high power—generally the 40× objective lens” (Fig. 5). It’s difficult, he said, to detect or quantitate the level of subtle expression at low or medium magnification using a 5× or 10× objective. “So detection of tumors with low levels of HER2 expression will require pathologists to spend more time with their cases.” For difficult cases, he recommends measures such as reviewing the case with a second pathologist for consensus.
Dr. Tozbikian shared three cases, each of which was scored independently by a panel of nine expert breast pathologists. Scoring was done on scanned whole slide images, and a consensus score was determined. The first case (Fig. 6) is a low-grade invasive lobular carcinoma. The consensus score was a 1+.“Looking at a static, fixed PowerPoint image is not the same as being able to evaluate the virtual slide,” he acknowledged, “but in this case, just looking at the specific focused high-powered field, you can see the staining pattern is membranous. But it’s largely incomplete. It’s not surrounding the entire circumference of the cell surface, in 360 degrees. That’s important. There’s only partial circumscription of the cells that show expression. Moreover, that expression intensity is weak. You have to use the 20× objective lens or even higher power to discern it.” At that power, the staining is dot-like. “It’s very granular, it’s faint, but it’s certainly present in greater than 10 percent of the tumor cells, at least in this field. Therefore this qualifies as a 1+.”
Case No. 2 (Fig. 7) is a grade three invasive ductal carcinoma, or non-special type, which the expert panel scored as 0. At 20×, scattered cells can be seen with barely perceptible membranous reactivity. “This staining is incomplete—it’s on only a portion of the cell membrane, and it’s very faint, very dot-like, sort of granular. And overall if you had to look at this field, these appear to represent at least less than 10 percent of the cells in this field. Assuming, of course, that the rest of the tumor stains in a similar fashion, this would qualify as a score 0.” It’s one of those examples where it’s not absent staining; there is some low level of expression, below that 10 percent threshold, he said, and therefore it is considered a score 0.
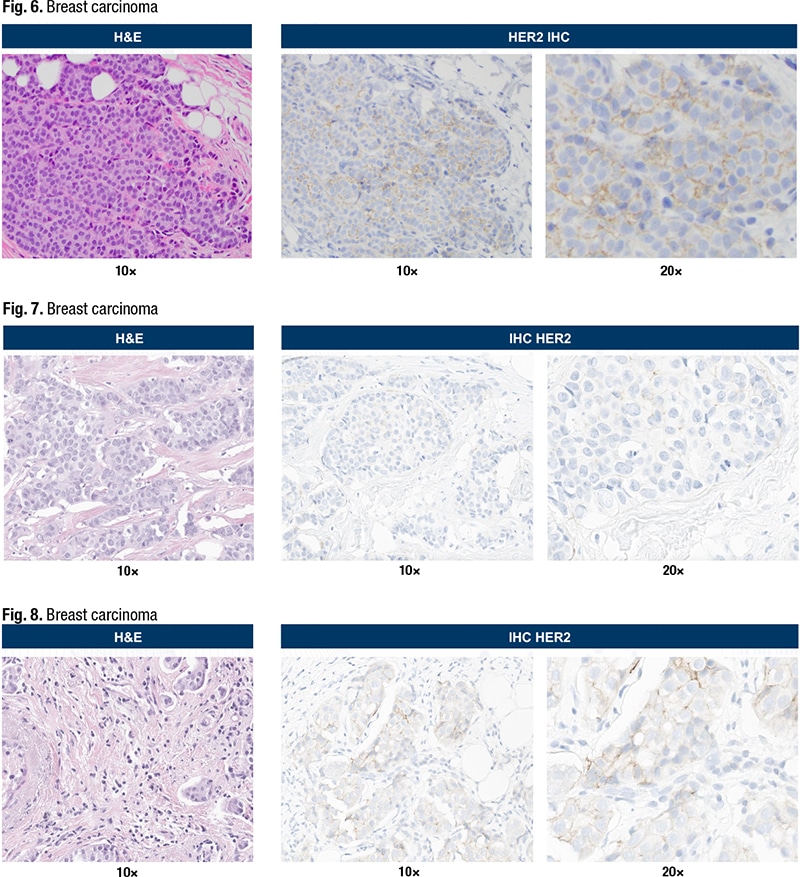
Case No. 3—“the most challenging of the three,” he said—is a grade two invasive ductal carcinoma, or non-special type tumor (Fig. 8). Using the 10× objective lens, membranous reactivity can be seen. “It’s detectable, it’s quite faint, but it’s much more readily seen at 20×. The majority of that membranous staining is, however, quite faint. There are a few scattered cells at the 12 o’clock location that show slightly stronger staining, slightly stronger membranous reactivity. But still appears incomplete. The percentage of cell staining is close to that 10 percent threshold or cutoff in this field.”
There were differences of opinion on this case among panel members. The consensus score was 1+, but a few pathologists in the group scored it as 0 and others scored it as a 2+. “So it just goes to show, at the lower ranges of expression, even under controlled conditions, it can be a challenge to achieve a perfect consensus,” Dr. Tozbikian said.
Sherrie Rice is editor of CAP TODAY.