
Sherrie Rice
December 2020—In an evaluation performed at Washington University in St. Louis and published recently, BioFire’s FilmArray pneumonia panel was found to have strong agreement with standard-of-care methods in identifying viral and bacterial targets in 200 lower respiratory tract specimens (Webber DM, et al. J Clin Microbiol. 2020;58[7]:e00343–20). It was also found to have strong agreement with the BioFire upper respiratory panel for common targets, making it unnecessary to perform both.
In comparison to standard-of-care methods, it has the potential to detect more Staphylococcus aureus and Haemophilus influenzae and to detect more antimicrobial resistance, particularly at low organism concentrations or in mixed cultures.
Those are the findings reported in a CAP TODAY webinar (captodayonline.com) on the implementation of multiplex PCR assays for pneumonia, made possible by a special educational grant from BioFire.
“Pneumonia is a clinical and diagnostic challenge because the etiologic agents can be variable, the conventional diagnostics are slow, and the long window of diagnostic uncertainty combined with the increase in antibiotic resistance can lead to overly broad spectrum empiric antimicrobial therapy,” Carey-Ann Burnham, PhD, D(ABMM), professor of pathology and immunology at Washington University and medical director of the Barnes-Jewish clinical microbiology laboratory, said in the Sept. 15 webinar.
“Interpretation of our diagnostic tests can be challenging,” she said, “because many of the bacteria that cause pneumonia are also common colonizers of the respiratory tract, and health care providers may need to order multiple diagnostic tests and laboratories may need to have available many methods for a comprehensive patient evaluation.”

The methods used today to diagnose bacterial pneumonia are culture based. In the laboratory at Barnes-Jewish Hospital, Dr. Burnham and Neil Anderson, MD, ABP-MM, D(ABMM), use qualitative culture for sputum and quantitative respiratory culture for other lower respiratory tract specimens, such as tracheal aspirate or bronchoalveolar lavage.
“We have multiple pieces of media with variable lengths of incubation. There is much interpretation required from our technologists,” said Dr. Anderson, assistant professor of pathology and immunology at Washington University and medical director of the Barnes-Jewish molecular infectious diseases laboratory, who co-presented and asked, “Is there a better way?”
The pneumonia panel and the BioFire upper respiratory pathogen panel have some targets in common, but “what’s new about the pneumonia panel are the 15 bacterial targets that are semiquantitative in nature,” Dr. Anderson said. Also new are the antimicrobial resistance determinants, both for Gram-positive organisms (such as mecA/C) and the multiple Gram-negative antimicrobial resistance determinants.
“This is a new and a different panel compared with what we have seen in the past,” he said, “and one of the things that’s new about it is the semiquantitative nature of reporting.” Bacterial organism abundance is estimated based on real-time PCR relative to an internal standard. Quantitation is reported in 1-log bins, ranging from 104 to ≥107 copies/mL.
Dr. Burnham, Dr. Anderson, and colleagues evaluated the pneumonia panel’s performance in comparison with standard-of-care testing. “We took 200 consecutively available lower respiratory specimens, collected from July 2018 to November 2019, with an entire flu season in that interval,” Dr. Anderson said. All patients had aerobic culture performed on their specimen and, depending on what the provider thought was necessary, a BioFire upper respiratory panel (RP2), a PCR test for other viral targets, and any other additional infectious disease workup as needed—all performed as part of standard-of-care testing.
They ran the BioFire pneumonia panel on the 200 specimens and compared the results of the panel with what was resulted from standard-of-care testing.
The average age of the patients was about 60, with a slight male predominance. “Some were immunocompetent, some were immunocompromised, some were in the ICU, some were in the ED. We had a good representation of different patients in our hospital,” Dr. Anderson said. Of the 200 specimens, 59 were bronchoalveolar lavage, 11 bronchial wash, 54 sputum, and 76 tracheal aspirate.
A viral or bacterial target was detected in 117 of the 200 specimens (58.5 percent), with more than one pathogen detected in 43 percent of the positive specimens. “So not only are many of these specimens positive, but many of the positives have multiple organisms detected.”

“The real question,” Dr. Anderson added, “is how this stacks up against the standard-of-care testing.” For the viral targets, there were nine instances of viral infections detected by standard-of-care testing for pathogens not on the pneumonia panel: five HSV and four CMV. “It is important to keep in mind that the panel doesn’t necessarily cover everything,” he said.
There were also nine instances of extra viral infections detected in which standard-of-care testing was not ordered. “These were cases in which the provider may have not been thinking about a viral etiology. But by running this broad panel, we were able to show positivity for a virus that may not have been suspected.” The clinical relevance of that detection depends on the situation, he noted, but in some of these cases, the finding may have been important.
When the target was tested for by standard-of-care methods and it was also in the pneumonia panel, they typically agreed.
For the bacterial targets, the story is similar, Dr. Anderson said. There were eight instances of bacterial detections by the standard of care for organisms not on the pneumonia panel, half of which were Stenotrophomonas maltophilia. (The others were Citrobacter freundii complex, Acinetobacter spp., Staphylococcus intermedius group, and Klebsiella variicola.) “However,” he said, “there were very few instances of standard-of-care positivity and BioFire negativity for the on-panel targets. If it was there by the standard-of-care method and it was included in the panel, the panel picked it up, suggesting a good negative predictive value.”
“What was interesting is that we had many instances”—92—“of unique pneumonia panel detections, the majority of which were Staphylococcus aureus and Haemophilus influenzae. One of our hypotheses,” he said, “was that perhaps these unique pneumonia panel detections were linked to either microorganism burden in the specimen and/or specimen type. So maybe there wasn’t enough there for the standard-of-care methods to detect it.”
For bacteria that were uniquely detected by the pneumonia panel, this was more common at low microorganism burden in the sample. “If there was not a lot of it there, it was more likely to be detected only by the BioFire.” For Staphylococcus aureus, the unique detections were more common in potentially polymicrobial specimens, such as sputum-type specimens. “It could potentially be that the S. aureus may be interpreted as part of normal microbiota in those specimen types and potentially overlooked,” Dr. Anderson said.
What is the significance of the unique pneumonia panel detections? Do they behave more like patients in which they were standard-of-care positive or patients in which they were standard-of-care negative?
They compared their sole detections to instances in which both methods were positive and instances in which both methods were negative, in terms of length of hospital stay and 30-day mortality, for S. aureus and H. influenzae. “The long and the short of it is that we didn’t have significant differences in length of stay or 30-day mortality for S. aureus or H. influenzae. However, our study wasn’t powered to answer this question, and it’s something that is in need of further research,” Dr. Anderson said.
When they looked at the methicillin-resistant S. aureus callout versus methicillin-susceptible S. aureus, the finding was similar. There was a lot of concordance, but the pneumonia panel detected more MRSA than culture. Eleven instances of MRSA detection were unique to the BioFire panel, and these were more common in polymicrobial samples. “The failure to recognize the resistant clone in mixed population in culture may explain these results,” Dr. Anderson said.
“We had a similar story when we looked at antibiotic resistance. When resistance was present, the pneumonia panel was very good at picking it up. We had great agreement between the pneumonia panel and standard of care in that regard. However, we did have 11 instances of unique detection of resistance in which a resistance organism was not identified by standard-of-care testing.”
In one instance, Klebsiella pneumoniae carbapenemase was detected in a tracheal aspirate. “By our standard-of-care method, this was called greater than 100,000 CFUs per mL of yeast and bacterial microbiota below the threshold for workup,” Dr. Anderson said. “The pneumonia panel gave results that also suggested a mixed population of microorganisms. We had Enterobacter cloacae and Pseudomonas aeruginosa, but we also had that KPC in there. I would argue that this is a very significant finding and a potential win for the pneumonia panel. For infection control implications alone, KPC is not something you want to miss.”
Dr. Anderson, Dr. Burnham, and colleagues compared the BioFire pneumonia panel to the BioFire upper respiratory panel when performed on the same specimen. “The reason we wanted to do this is because our lab, similar to many other labs, has validated the BioFire upper respiratory panel for off-label testing on lower respiratory specimens. There aren’t a lot of options for broad pathogen testing of lower respiratory specimens, so we have been using the upper respiratory panel for this purpose following appropriate validation.”
“Now that we have a large panel for lower respiratory testing, is it necessary to run both?” he asks. “Is there one that’s better than the other for specific targets, and, if so, we want to know that so we can adjust our workflow appropriately.” They tested the 200 specimens by the BioFire upper respiratory panel (RP2) and compared that to the pneumonia panel results. “We wanted to make sure we were comparing apples to apples, so both of these tests were performed on exactly the same specimen and then we just simply compared results.” There was strong agreement between both panels, with only eight discrepant results out of the 200 samples tested, for a 96 percent overall agreement for targets common to both panels.
Does the discrepant analysis favor one assay versus the other? “The short answer is no,” he said. “We had unique detections in favor of the pneumonia panel, and we had unique detections in favor of the upper respiratory panel. So this can be interpreted as there not being any difference in performance for the shared targets between the two panels. And that translates to no benefit in performing both assays in parallel on the same specimen. That’s an important piece of data we all need to keep in mind when we put together our workflows.”
The final data Dr. Anderson reported was the projected improvement in turnaround time with the pneumonia panel. Their study found it took about 44 hours to get an organism identification and another 14 hours to get phenotypic susceptibility testing with conventional methods. When they run a pneumonia panel, results are out in about 2.3 hours following specimen receipt. “In our study we performed the pneumonia panel retrospectively, so the estimated turnaround time was based on RP2.0 [upper respiratory pathogen panel] testing.”
“This is an estimated 42-hour savings in the amount of time it takes to turn around an organism ID, and a 56-hour savings in how long it takes to turn around a susceptibility.”
Dr. Burnham cited a study published this year that estimated the potential impact of the finding of good analytical performance characteristics for the pneumonia panel compared with standard-of-care methods on early modification of antibiotic therapy (Buchan BW, et al. J Clin Microbiol. 2020;58[7]:e00135–20). “And I say potential impact because this was theoretical based on retrospective review,” Dr. Burnham said.
“The findings were striking although not entirely surprising,” she said. “They found that in nearly half of patients that antimicrobials could be appropriately de-escalated or discontinued based on having the result more quickly. In a small proportion of patients, about four percent, the antibiotics should have been escalated or initiated, and although that’s a relatively small number of patients, I think that’s really important. We know that if there are delays in appropriate therapy, outcomes are compromised.”
Which antimicrobials had the most opportunities for adjustment? “Given that so much S. aureus is methicillin resistant, it’s not at all surprising to me that vancomycin was the biggest offender, where we had the most opportunities for making earlier adjustments.” Appropriate antibiotic de-escalation/discontinuation of piperacillin/tazobactam was the next largest category of possible adjustment opportunities.
The group compared the bacterial quantification from the pneumonia panel to the standard-of-care culture result, and for many of the samples, the pneumonia panel result was about a log higher than the standard-of-care result. “This is similar to what we saw in our study presented by Dr. Anderson, so it is important for the laboratory and for health care providers to keep in mind that the quantification is probably going to be about one log higher using the pneumonia panel compared to conventional culture,” Dr. Burnham said.
“How should labs think about this in the context of COVID?” she asked, noting that both studies were performed pre-pandemic. For other important respiratory pathogens, such as influenza, bacterial coinfection is often what contributes to the morbidity and mortality and it has been documented that empiric antibiotic use is common in COVID patients who are admitted to the ICU. “So this is a great example where the negative results for the bacterial targets could be very clinically useful in some patient populations,” she said, “both in terms of the bacterial pathogens and the resistance genes, to drive some of mostly the de-escalation that we talked about in a prior study.”
Up next: how to take the pneumonia panel from evaluation to implementation. “One of the most important questions that needs to be answered at the outset,” Dr. Anderson said, “is who you are going to test.” The patient populations commonly tested using lower respiratory specimens, when seeking a diagnosis of pneumonia or a respiratory infection, are community-acquired pneumonia patients, ventilator-associated pneumonia patients, and patients living with cystic fibrosis. For patients with community-acquired pneumonia, the laboratory typically receives a lower respiratory tract specimen, such as a sputum, BAL, or a bronchial wash. “Most of the important pathogens are on the panel for those patients,” he said.
“It’s a little more complicated for our ventilator-associated pneumonia patients. Certainly we get lower respiratory tract specimens, though we often get specimens like tracheal aspirates.” While the majority of common pathogens in that patient population are on the panel, he said, “Stenotrophomonas maltophilia is an important pathogen in those patients, at least in our hospital, and that’s not on the panel. So there are some gaps for these patients. However, they do need rapid results, so one could argue a BioFire pneumonia test in those patients could still be of great benefit.”
For patients living with cystic fibrosis, Dr. Anderson said, the story is a bit different. “The predominant specimen type we get from those patients is sputum, so not necessarily the clean lower respiratory specimen like a BAL or bronch wash.” Stenotrophomonas maltophilia here, too, is a gap, but the Burkholderia cepacia complex organisms are one of the most important pathogens in cystic fibrosis patients and those aren’t on the panel either. “So you’re still going to need the culture for those patients,” he said. “Another thing to keep in mind is for patients with cystic fibrosis, a lot of specimens are collected on an outpatient basis; there isn’t a lot of urgency in working those up, so maybe there is less of a benefit in a rapid test.”
Explaining that he is not trying to be prescriptive in any way, Dr. Anderson said hospitals, laboratories, and providers do need to think about if there are patients who should never be tested by this panel or patients who should always be tested by the panel. Dr. Burnham said the laboratory can help drive appropriate testing and “can have various levels of flexibility in that approach.” It can be orderable by all providers or only by certain providers.
“You might also think about it from a patient population-based approach,” she said, whereby it is orderable only for certain patients, populated into order sets for relevant patients, or automatically added to lower respiratory cultures for relevant patients. “Although I think the pneumonia panel always needs to be coupled with a culture, a culture does not always need to be coupled with a pneumonia panel,” Dr. Burnham said.
Other approaches to driving appropriate testing are to make it location based (for patients in the ICU, for example) or service-line–based (lung transplants).
A[/dropcap] potential issue with the pneumonia panel is unnecessary repeat testing, Dr. Anderson said. He and colleagues at Barnes-Jewish Hospital quantified repeat testing for viral respiratory pathogens over 30 months, from March 2013 to September 2015 (Qavi AJ, et al. J Appl Lab Med. 2020;5[5]:897–907).
They were running two different assays for respiratory testing at that time: influenza PCR (Cepheid) and the BioFire upper respiratory pathogen panel. They defined repeat testing as testing ordered within seven days of a prior test. “No surprise here—we had a lot of repeat testing. At first it might not seem like it’s that much. We had 10,198 flu tests performed and only three percent of those are repeats, but that correlates to about 293 repeat influenza PCRs.”
For the upper respiratory pathogen panel, 12,536 were performed and 10 percent were repeats.
They quantified repeat testing further and found concerning trends. “There are a lot of instances of patients getting greater than four tests within that seven-day period. Even more concerning is most of our repeat testing was occurring within a single day. And when we drilled down even closer, we found that 10.8 percent of our repeat flu assays were ordered within eight hours of the previous one, and 20 percent of our repeat respiratory pathogen panels were ordered within eight hours of the previous one. That’s important because eight hours is the test turnaround time we quote to our providers.”
That tells him and his colleagues that repeat testing in many instances is being ordered because of confusion. “It’s being ordered without knowledge of a prior pending result or a prior result,” he said, “and one could ask what the yield was of the repeat testing.
“We looked at the amount of times you had an initial negative and it became positive, because one could argue that’s where you would see the benefit. That rarely occurred,” he continued. “That happened only 2.7 percent of the time with the flu repeats and six percent of the time with the respiratory pathogen panel repeats. So only very rarely were we getting useful information.”
They looked, too, at specimen type (271 patients with BAL and NP swab). “We found similar results, in that there were very few instances where you had discrepant results. So very rarely did we ever get additional information that was helpful.”
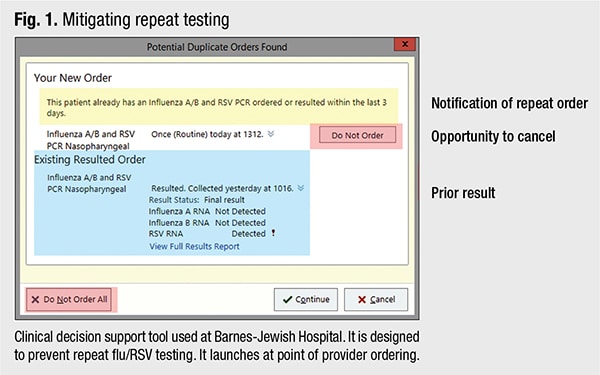
They set out to mitigate the problem by implementing a clinical decision support tool, in collaboration with their lab information system experts, to prevent repeat flu/RSV testing (Fig. 1). Providers are given the prior result and multiple opportunities to cancel the order. “One can think of a lot of different ways to potentially implement something like this for the pneumonia panel,” Dr. Anderson said.
How can labs incorporate this method into their existing methods for pneumonia diagnosis?
“Whether reporting thresholds should be used is a major question,” Dr. Anderson said. The package insert says detection of bacterial nucleic acid may be indicative of colonizing or normal respiratory flora and may not indicate the causative agent of pneumonia. What to do with that?
“We use cutoff thresholds with quantitative culture,” he said. Could something similar be done with the pneumonia panel? “A lot of the sole detections occur at lower amounts of bacteria. One could imagine implementing cutoffs to make the pneumonia panel results more in line with what you would expect to see with culture. This is something that individual laboratories need to consider and potentially think about adopting based on data from their own validations.”
Another question: What role is the Gram stain going to play in evaluating specimens for adequacy? The package insert says institutions should follow their own established rules for acceptance or rejection of sputum specimens—for example, using Gram stain or Q-score—and therefore apply appropriate guidelines locally for acceptance and rejection. “In other words, you probably need to continue to do your Gram stain,” Dr. Anderson said.
The Washington University study found a higher amount of detection of S. aureus in sputum-type specimens. Those were specimens that were acceptable for culture. “We routinely reject about a quarter of our sputum specimens because they have unacceptable Gram stains for culture. So one could imagine what these results would look like if we ran the pneumonia panel on all of those specimens.”
It wouldn’t be surprising, he said, to see more S. aureus in those specimen types. “That study remains to be done, but it could be potentially misleading. This is something people need to keep in mind.”
Using the Gram stain criteria for other specimen types is another thing to consider, Dr. Anderson said. “Tracheal aspirates have the potential to be very mixed and polymicrobial, and a laboratory might want to consider avoiding doing the pneumonia panel on these mixed specimens.”
Dr. Burnham said it’s important to pair the pneumonia panel with bacterial culture. “When you do a molecular test you only get what you look for,” she explained, “and while the molecular panel is well designed and comprehensive, there is limited real estate on the multiplex panel. By doing bacterial culture, you might detect something that was not available to be detected on the pneumonia panel, and depending on your patient population this will have different levels of importance.”
Some of the bacterial targets are resolved to genus or complex, or group if desired. And then there’s the ability to perform antimicrobial susceptibility testing. “While the pneumonia panel does have important resistance targets, they can help inform resistance, but a phenotypic susceptibility is still required to finalize patient treatment,” she said.
How to best report the results is the next question, and “with all the experience labs have with rapid diagnostics for positive blood cultures,” Dr. Burnham said, “there’s no need to reinvent the wheel.”
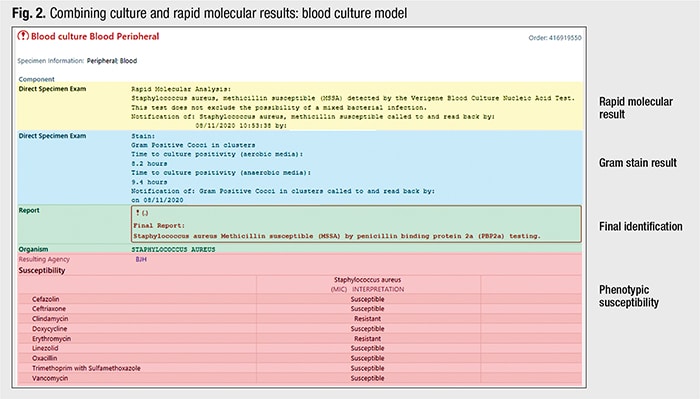
She and colleagues have incorporated molecular results with positive blood culture results (Fig. 2). “We have a rapid molecular result, and it’s not just a list of organisms and targets. We have interpreted it. For example, it’s S. aureus and methicillin susceptible. We also include the result of the Gram stain and what grew in the culture, in this case Staphylococcus aureus, and what the phenotypic susceptibility results listed.” Also reported are resistance determinants.
“So the results of the bacterial components of the molecular test and the phenotypic tests are in one place, and the physician can see them and interpret them all together.” The laboratorian who is working on it, too, can see it and interpret and work up the culture in the context of the rapid molecular result. “This is not to say all components need to be reported this way,” Dr. Burnham said. “Some laboratories may choose to take this strategy with bacterial results that can be linked to culture, while reporting the viral targets separately as discrete results. Clinical decision support should also play a role in reporting.”
“You need to consider,” Dr. Anderson added, “how instructive reporting comments, active reporting, coordination with your clinical pharmacy, and coordination with antimicrobial stewardship can affect the utility of the test.”
Perhaps their most important message is that laboratories should not attempt to implement a test like the BioFire pneumonia panel in a vacuum. They should engage with clinical, laboratory, and informatics experts, Drs. Anderson and Burnham say, to realize the panel’s maximum benefit.
Sherrie Rice is CAP TODAY editor. The Washington University study used BioFire RP2. RP2.1 includes SARS-CoV-2.